
Open Access, Volume 10
The hidden truth from mycosis fungoides to NK T-Cell lymphoma: A case report
Ahmed Medhat Eldimllawi1#; Islam Samir Elkonaissi2#; Fatima Ahmed Abdullah Al Hasani3; Mohamed A Osman4; Aseel Suleiman Mohieldin Al-Sayed1; Husni Alhateeti1; Kayane Mheidly1*
1Hematology Department, Sheikh Shakhbout Medical City, Abu Dhabi, UAE.
2Senior Clinical Pharmacist, Sheikh Shakhbout Medical City, Abu Dhabi, UAE.
3Pharmacy Alumnus, Fatima College of Health Sciences, Abu Dhabi, UAE.
4Pathology Department, Sheikh Shakhbout Medical City, Abu Dhabi, UAE.
#Co-first authors.
Kayane Mheidly
Hematology Department, Sheikh Shakhbout Medical City, Abu Dhabi, UAE.
Tel: 0097-150-855-2956;
Email: Mheidlykayane@yahoo.fr
Received : September 04, 2024,
Accepted : September 23, 2024
Published : September 27, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: Cutaneous T-Cell Lymphomas (CTCLs) make up 70% to 82% of all primary cutaneous lymphomas, with Mycosis Fungoides (MF) accounting for about the half. Extranodal NK/T-Cell Lymphoma (NK/TCL) is a rare aggressive type of lymphoma, often involving the nasal cavity. NK/TCL is typically fatal, while MF follows an indolent course. We report a rare case of a patient with a known history of MF, who has developed central nervous system NK/T-cell lymphoma.
Case presentation: A 50-year-old female with refractory MF developed erythematous, papular lesions on the nose, progressing to necrosis. Lesions expanded despite antimicrobial therapy. Biopsies confirmed MF. Treatment with methotrexate, steroids, psoralen Plus Ultraviolet A (PUVA) therapy, and anti-CC chemokine receptor 4 therapy yielded suboptimal responses. Total skin electron beam therapy and antibody-drug conjugate anti-CD30 infusions were also administered with unsatisfactory results and complicated by respiratory infections and osteoporotic vertebral fractures. In October 2023, left-sided facial palsy prompted further investigations revealing NK T-Cell lymphoma cells involvement in the lumbar puncture. The unexpected NK/T-cell lymphoma diagnosis in a patient initially diagnosed with MF suggests dual pathology. After cycles of chemotherapy regimens and programmed cell death-1 inhibitor, multiple repeated cerebrospinal fluid analyses showed no evidence of NK-T cells. A remaining ulcerating skin lesion with regular borders on her right leg was biopsied with no evidence of MF.
Conclusion: The coexistence of MF and NK/T-cell lymphoma opens avenues for research into their potential associations and shared etiopathogenic mechanisms. Thorough pathological assessments and vigilant monitoring are crucial for accurate diagnosis and optimal management.
Keywords: Mycosis fungoides; Cutaneous T-cell lymphoma; Lymphoma; NK T-cell lymphoma.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Mheidly K (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Eldimllawi AM, Elkonaissi IS, Al Hasani FAA, Osman MA, Alhateeti H, Mohieldin Al-Sayed AS, Mheidly K, et al. The hidden truth from mycosis fungoides to NK T-Cell lymphoma: A case report. Open J Clin Med Case Rep. 2024; 2288.
Introduction
Primary cutaneous lymphomas are classified into two main types by the World Health Organization (WHO) and the European Organization for Research and Treatment of Cancer (EORTC): Cutaneous B-Cell Lymphoma (CBCL) and cutaneous T-cell lymphoma (CTCL) [1]. Of these, CTCLs predominate as they account for between 70% and 82% of all primary cutaneous lymphomas. Mycosis Fungoides (MF) is the most common type of CTCL, making up approximately half of all primary cutaneous lymphomas [2]. Although the exact cause of MF is still unknown, factors such as genetics, environment, and infectious agents (e.g. infection with the human T-cell leukemia virus 1) have been linked to the activation or transformation of lymphocytes [3]. Prognosis and treatment depend on the stage and specific characteristics, with therapies ranging from skin-directed to systemic treatments, including innovative approaches like allogeneic bone marrow transplantation and extracorporeal photopheresis [4].
Nasal-type extranodal Natural Killer/T-Cell Lymphoma (NK/TCL) is an uncommon and aggressive form of lymphoma with a predilection for the nasal cavity. Extranasal involvement is also reported, with the skin being the most frequent site [5]. NK/TCL is classified as a CTCL in the current WHO/EORCT classification of skin tumors (2018) [1] and as Epstein-Barr virus-positive NK/T-cell lymphomas in the recent WHO classification of hematolymphoid tumors (2022) [6]. From a histopathological perspective, the dermis and subcutis in NK/TCL contain diffuse populations of small, medium-sized, or large atypical lymphocytes with evident epidermotropism in some cases [7].
It is important to distinguish between MF and other cutaneous lymphomas exhibiting epidermotropism because the prognosis of these conditions differs significantly; NK/TCL usually has a fatal course, while MF follows an indolent course [1,8,9]. Distinctions are also observed between the two in their immunophenotype: Generally, NK/TCL atypical lymphocytes are marked by CD56, TIA-1, granzyme-B, perforin-A, and CD3ε (cytoplasmic), while the expression of CD4 or CD8 varies. Crucially, NK/TCL should exhibit positive in-situ hybridization for Epstein-Barr virus-Encoded RNA (EBER) [10,11]. By contrast to NK/TCL, the atypical lymphocytes in MF frequently express CD3 and CD4, but do not express CD8, CD56, or TIA-1 [1].
Reaching a correct diagnosis is critical for effective management, yet remains challenging due to overlapping disease presentation and the need to correlate clinical, immunophenotypic, histopathological, immunohistochemical, molecular and genetic findings as none are individually sufficient for diagnosis. Published reports have previously described cases of NK/TCL mimicking MF [12], and inversely, subtypes of primary CTCLs mimicking NK/TCL [13,14]. However, there have been no previous reports of concurrent MF and NK/TCL to the best of our knowledge. We herein report a rare case of a patient with a known history of MF, who has developed Central Nervous System (CNS) NK/TCL.
Case Presentation
A 50-year-old female initially presented with a history of seborrheic dermatitis. In 2020, a stable skin lesion was observed on the patient’s upper back. By November 2021, erythematous, papular lesions appeared on her arms, nose, and cheeks (Figure 1.1a-f), with subsequent necrosis on the left nasal side. The patient did not exhibit any B-symptoms (such as fever, or night sweats) and skin lesions were initially thought to be related to mask friction due to prolonged occupational wear (face mask worn as a precautionary measure during the COVID-19 pandemic as the patient was a healthcare worker). A Culture from the facial lesions was positive for Klebsiella and the patient was started on doxycycline, metronidazole, and later ciprofloxacin. However, the facial lesions continued to expand despite antimicrobial therapies.
In July 2022, a dermatological evaluation at hospital revealed bilateral indurated erythematous patches on the cheeks, a swollen nose with necrotic eschar, and an eczematous plaque on the upper back (Figure 1.2a-b).
Magnetic Resonance Imaging (MRI) of the paranasal sinuses was also done in the same month and showed anterior nasal cavity soft tissue wall thickening and enhancement, somewhat nodular. Neither gross necrotic changes and nor deeper extension were observed. No orbital, skull base, or intracranial involvement. The rest of sino-nasal cavity was clear. Upper neck showed bilateral enlarged lymph nodes and the left submandibular lymph nodes were up to 4 cm. In July 2022, two punch biopsies from left cheek and right flank were taken from the patient. After multiple reviews from different pathologists and multiple addendums, we reached the final diagnosis of MF with folliculotropism in October 2022. Cytological count on peripheral blood for Sezary cells was not requested.
Blood flow cytometry showed no significant downregulation of pan-T-cell antigens (CD7+ = 0.7%; CD2+ = 0.4%) as seen in reactive conditions (Figure 1.3). Additional flow cytometry markers such as CD26 to confirm Sezary cells was not available in our facility. TCR rearrangement on peripheral blood was not done.
Positron Emission Tomography Computed Tomography (PETCT) scan was conducted in October 2022 for disease staging and to assess the presence of any systemic disease. Multifocal extensive Fluorodeoxyglucose (FDG) avid cutaneous/subcutaneous infiltrative nodularities were observed in keeping with MF. The skin lesions were FDG avid except for the left alar nasal lesion. No FDG avid visceral deposits were observed. After all these investigations, we concluded that this is a case of MF with a TNM staging of T1bN0M0.
In November 2022; patient was started on systemic corticosteroids, psoralen Plus Ultraviolet A (PUVA) therapy, and subcutaneous methotrexate without any improvement. In January 2023, the patient had intraoral ulcer on the left side of the palate which was severely painful and affected her ingestion (Figure 1.4). A biopsy of this lesion confirmed MF in oral palate with TCR rearrangement.
In March 2023, patient developed new lesions on her face and scalp (Figure 1.5); the patient was switched to anti-CC Chemokine Receptor 4 (anti-CCR4) therapy and completed two cycles. After starting anti CCR4, the erythematous patches on the back did not improve (April 2023) (Figure 1.6). The patient received one dose of the third cycle after which it was stopped due to rash which presented as generalized erythematous patches (last dose was on the 20 of June 2023). After that, the patient progressed and developed multiple plaque-like lesions over her face with some ulceration on her nasal tip and cheeks. The lesions were erythematous and ulcerated. There were numerous lesions over forehead cheeks, nose, and lower face.
Several biopsies were repeated. Skin biopsy from left forearm, right shoulder, and from the back showed atypical lymphocytic proliferation consistent with patient’s known MF. No large cell transformation was identified in the current biopsy. The peripheral blood flow cytometry showed no evidence of Sezary cells in this significant lymphocytopenia background.
After plan discussion, the patient was presented to radiotherapy team and a partial electron beam therapy to her face and hard palate lesions was decided but not available in the UAE. In June 2023, the patient travelled abroad for treatment and received 12 cycles of Total Skin Electron Beam Therapy (TSEBT): 6 cycles for the total skin, and 6 cycles for targeted lesions/areas in addition to two cycles of an antibody-drug conjugate anti-CD30.
In September 2023, clinical examination showed poor Eastern Cooperative Oncology Group (ECOG) Performance Status (PS score of 3) with fever (38.5°C), chills, a diffuse skin rash with itching, and painful ulcerative oral lesions. Laboratory investigations revealed positive blood and urine cultures for E. coli, and the patient also tested positive for COVID-19. A CT scan of the chest showed multiple bilateral nodular lesions of varying sizes, with the largest in the right lower lobe measuring 3x2 cm and another significant lesion in the left perihilar region of the upper lobe measuring 2.3x2 cm, which was biopsied (Figure 1.7a-d).
In September 2023, disease progression causes the patient to present to the Emergency Department in UAE with almost generalized skin rash and back pain, rash associated with significant itching (Figure 1.7e 1.7f). Biopsy of the hilar lymph nodes confirmed a diagnosis of MF, with more than 10% skin involvement. The TNMB staging was T3N3M0B0, with negative results for TCR rearrangement and clonality. An MRI on the same date identified multiple vertebral compression, a 1.5 x 0.7 cm focus of T2 hyperintensity in the left corona radiata likely representing fractures gliosis, but no acute infarct, intracranial hemorrhage, mass, or midline shift. Additionally, the patient has spondylotic changes and multiple endplate fractures.
In October 2023, the patient developed left-sided facial paralysis, and her condition deteriorated, resulting in ECOG PS score of 3, grade 2 mouth mucositis, and extensive ulcerative skin lesions covering over 50% of her body surface area. An MRI of the brain showed focal thickening and enhancement of the canalicular and tympanic segments of the left facial nerve and adjacent vestibulocochlear nerve, without suspicious intra-axial enhancement. A tiny hemosiderin deposit was noted in the left frontal lobe.
Cerebrospinal Fluid (CSF) flow cytometry after a lumbar puncture showed 91.5% of cells with a NK cell immunophenotype, leading to a diagnosis of NK/T-cell lymphoma in addition to her existing MF (Figure 1.8a-b). Following a multidisciplinary discussion, chemotherapy with one cycle of CHOEP regimen (cyclophosphamide, doxorubicin, etoposide, vincristine, and prednisone) and intrathecal methotrexate were started. She was then switched to a modified SMILE regimen (dexamethasone, high-dose methotrexate, ifosphamide, L-asparaginase, and etoposide), in addition to two doses of a programmed cell death-1 inhibitor and intrathecal methotrexate. Multiple repeated CSF analyses showed no evidence of NK-T cells. A remaining ulcerating skin lesion with regular borders on her right leg was biopsied and showed no evidence of MF. The nasal and cheek lesions had also resolved (Figure 1.9a-d).
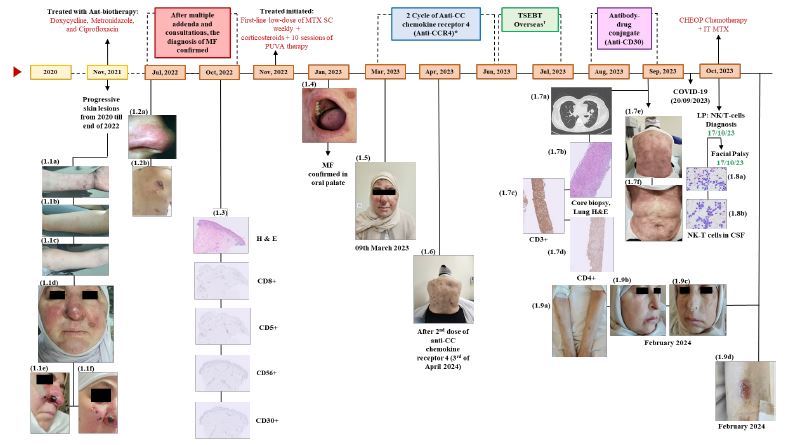
Figure 1: Timeline of the diagnosis and treatment of mycosis fungoides and NK/T Cell lymphoma.
CHEOP: Cyclophosphamide, Doxorubicin, Etoposide, Vincristine, and Prednisone; CSF: Cerebrospinal Fluid; H&E: Hematoxylin and Eosin; IT: Intrathecal; LP: Lumbar Puncture; MTX: Methotrexate; NK: Natural Killer; PUVA: Psoralen Plus Ultraviolet A; S/C: Subcutaneous; TSEBT: Total Skin Electron Beam Therapy.
*Third cycle: One dose then stopped due to rash - Last dose 20th June 2023.
†Two doses only on 06/06/2023 and 20/06/2023.
CHEOP: Cyclophosphamide, Doxorubicin, Etoposide, Vincristine, and Prednisone; CSF: Cerebrospinal Fluid; H&E: Hematoxylin and Eosin; IT: Intrathecal; LP: Lumbar Puncture; MTX: Methotrexate; NK: Natural Killer; PUVA: Psoralen Plus Ultraviolet A; S/C: Subcutaneous; TSEBT: Total Skin Electron Beam Therapy.
*Third cycle: One dose then stopped due to rash - Last dose 20th June 2023.
†Two doses only on 06/06/2023 and 20/06/2023.
Discussion
The detection of NK/TCL, typically CD30 positive [15], in a patient initially diagnosed with CD30-negative MF, suggests the presence of dual pathology or a possible transition from one lymphoproliferative disorder to another.
The three clinical phases of MF are patch, plaque, and tumor stage. The disease’s course is typically indolent and spans several years or decades. Over 90% of individuals with early-stage MF are thought to never reach the tumor stage and never exhibit extra cutaneous disease symptoms [1,8]. Because early MF presents with a wide range of clinical and pathologic manifestations, diagnosis is frequently challenging [16]. Diagnostic delays are reported in the majority of patients, with a median delay of 36 months (3 years) from first symptom development until initial diagnosis [17]. Consistently, proper diagnosis of the presented case required almost 2 years and consultation of many physicians (including dermatologists and hematologists).
Early MF may histopathologically resemble long-term inflammatory dermatoses involving reactive T cells and other immune cells [18]. Correlation of clinical and pathologic findings is essential for early MF diagnosis due to the difficulty of the diagnosis; Multiple follow-up skin biopsies are usually necessary to establish a histological diagnosis of early MF disease [19], and should be conducted after stopping all the topical treatment and corticosteroids treatment. Novel immunohistochemical and molecular biology techniques, notably TCR rearrangement, have been recognized as an adjunct test that can support MF diagnosis and its differentiation from benign conditions [20]. The patient in the presented case was diagnosed with MF based on punch biopsy conducted after development of a necrotic nasal lesion. Multiple biopsies were done and were subsequently examined by experienced histopathologists in dermatology and lymphomas diseases. This was in accordance with current clinical guidelines, which recognize the importance of correctly diagnosing and staging MF as a fundamental step for selection of the optimal therapeutic approach [21,22]. Staging and classification typically follows the Tumor (skin), Lymph nodes, Metastasis (viscera) Blood (TNMB)-staging classification. The treatment of MF is usually done in an incremental (step-wise) strategy that is adapted to the disease stage, and remains largely palliative. While curative treatment is rarely possible, appropriate treatment will prove effective in most cases. To achieve disease control, treatment of MF usually relies on skin-directed therapies, alone or in combination with systemic therapies for more advanced cases. Skin-directed therapies, which include topical agents, phototherapy and radiation therapy, are the most commonly used therapy for the first-line management of MF and have an overall response rate of 73% [23]. By contrast, systemic therapies (such as retinoids, chemotherapy, Histone Deacetylase (HDAC) inhibitors, brentuximab, and mogamulizumab) are used for advanced disease stages and have a lower overall response rate when used in the first-line setting (57%) [23].
Despite the histopathological confirmation of MF from skin biopsies in the presented case, the patient exhibited a clear lack of response to multiple lines of standard therapeutic modalities, including PUVA, CCR4 inhibition, and TSEBT. The persistence and progression of the disease despite aggressive treatment are atypical for MF, which generally responds to such interventions, especially in the earlier stages (response rates ranging from 84.6% to 100% for PUVA [24], and 76% to 93% for TSEBT [25]. The resistance to treatment, in this case, suggests either an unusual variant of MF with aberrant molecular pathways conferring treatment resistance or the coexistence of another pathologic process that was initially overlooked. Furthermore, the diagnosis of cutaneous lymphoma should be suspected if topical therapy does not work after 2 weeks. To make matters worse experts in cutaneous lymphoma has suggested that topical corticosteroids and other skin direct therapies should be on hold ≥2 weeks [26-28].
The most unexpected development in the case was the presentation of the patient with left-sided facial palsy. Imaging studies, including MRI, revealed thickening and enhancement of the left facial and vestibulocochlear nerves, indicative of possible lymphomatous involvement. CSF flow cytometry after lumbar puncture surprisingly showed 91.5% of cells with an NK cell immunophenotype, leading to the diagnosis of NK/TCL.
Nasal type extranodal NK/TCL is an uncommon aggressive non-Hodgkin’s lymphoma that grows quickly. Although it can originate in T cells, NK cells are typically where it develops [29,30]. Primary CNS extranodal NK/TCL is an extremely rare condition, with less than 25 cases reported in English literature [31]. Pathological diagnosis of primary CNS extranodal NK/TCL is a necessary step for ruling out invasive and secondary NK cell leukemia. Cases previously reported indicate that patients with primary CNS extranodal NK/TCL have a low overall survival rate of around 6 months (highest survival recorded was 139 months) [28,31-33].
To the best of our knowledge, the association CTCL with NK/TCL lymphoma has never published prior to this case. Nonspecific clinical symptoms like headaches, dizziness, vomiting, and blurred vision are frequently present with NK/TCLs. Loss of vision acuity and limb weakness were the initial symptoms in our patient, which was in line with the vague signs of primary CNS lymphoma. Histologically, published cases of primary CNS extranodal NK/TCL revealed vascular-centered infiltration along with vascular damage and necrosis. Several markers were expressed almost ubiquitously, including CD3 (95.2%; 20/21), CD45 (100%; 6/6), EBER (100%; 18/18), and cytotoxic molecules (TIA-1/granzyme B/perforin) (100%; 12/12), with lesser expression of others such as CD56 (75%; 15/20) and CD5 (12.5%; 1/8). Moreover, T cell clonality is variable and can be observed in as little as half and as many as most of NK/TCLs [30,31,34]. Similarly, in our patient, CSF flow cytometry analysis revealed sheets of medium to large neoplastic cells characterized by basophilic and predominantly angular cytoplasm, coarse chromatin, and inconspicuous nucleoli. But in our case the analysis showed 100% lymphocytes. T cells were 30% of all nucleated events with a CD4:CD8 ratio of 0.45:1. Double CD4/CD8 negative T-cells were 4.2%. NK cells accounted for 70% and were positive for CD2, CD7, CD26, and CD45. These cells were negative for CD3, CD4, CD8, and CD28.
A review off all the biopsies conducted for the patient confirmed the coexistence of 2 lymphomas, namely CTCL based on the skin biopsy and NK/TCL in the CNS. As our patient presented with the CNS involvement features, she was started on systemic chemotherapy to ensure concurrent management of CTCL and CNS NK/TCL. Chemotherapy regimens (drug combinations) such as DDGP (dexamethasone, cisplatin, gemcitabine, and peg-asparaginase) and SMILE (dexamethasone, methotrexate, ifosphamide, l-asparaginase, and etoposide) are typically used to treat nasal type extranodal NK/T-cell lymphoma [33,35]. Chemotherapy with CHOEP (cyclophosphamide, doxorubicin, etoposide, vincristine and prednisone) and intrathecal methotrexate were initiated. Subsequently, the patient was then switched to the modified SMILE (dexamethasone, steroid, methotrexate, ifosphamide, L-asparaginase, and etoposide) protocol combined with a programmed cell death-1 inhibitor after a comprehensive multidisciplinary team discussion.
Conclusion
In conclusion, the overlap of clinical features and the rarity of a subsequent NK/T-cell lymphoma diagnosis in a patient with an existing CTCL diagnosis presents a unique clinical challenge and underscores the importance of a thorough pathological assessment. This intricate medical narrative highlights the complexities involved in diagnosing and managing cutaneous T-cell lymphomas, shedding light on the importance of vigilant monitoring and adaptive treatment strategies. Moreover, this unique case encourages further research into potential associations and shared etiopathogenic mechanisms between these two rare lymphomas. The findings provide valuable insights into the diagnostic intricacies and treatment strategiesfor such complex cases, urging healthcare professionals to maintain a high index of suspicion and conduct thorough pathological assessments for accurate diagnosis and optimal patient management to improve outcomes.
Declarations
Funding: Nancy Al Akkary, BSc, MSc and Mohammad Yassine, BPharm, MSc, from Phoenix Clinical Research, Lebanon provided medical writing assistance for the preparation of this manuscript; the medical writing fee was funded by Kyowa Kirin. The views and opinions expressed are those of the authors only.
Conflict of interests: All the authors declare having no conflict of interests.
Ethics approval: Not applicable.
Consent to participate: Consent to participate was not required since this report describes a case from routine clinical practice.
Consent for publication: Informed consent was obtained from the patient for the publication of the present case report.
Availability of data and material: Not applicable.
Code availability: Not applicable.
Author contributions: All authors were involved in the conception, design, drafting and final approval of the case report. All authors agree to be accountable for all aspects of the work.
Acknowledgements: The authors thank Nancy Al Akkary, BSc, MSc and Mohammad Yassine, BPharm, MSc from Phoenix Clinical Research, Lebanon for providing editorial and medical writing assistance for the preparation of this manuscript. This medical writing fee was funded by Kyowa Kirin.
References
- Willemze R, Cerroni L, Kempf W, Berti E, Facchetti F, et al. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood. 2019; 133(16): 1703-14.
- Gallardo F, Pujol RM. Genetics Abnormalities with Clinical Impact in Primary Cutaneous Lymphomas. Cancers. 2022; 14(20): 4972.
- Girardi M, Heald PW, Wilson LD. The Pathogenesis of Mycosis Fungoides. N Engl J Med. 2004; 350(19): 1978-88.
- Kamijo H, Miyagaki T. Mycosis Fungoides and Sézary Syndrome: Updates and Review of Current Therapy. Curr Treat Options Oncol. 2021; 22(2): 10. Available from: https: //doi.org/10.1007/s11864-020-00809-w
- He L, Zou Y, Tang X, Wang J, Xing L, et al. Survival trends for extranodal NK/T-cell lymphoma, nasal type from different anatomical sites: a population-based study. Ann Transl Med. 2021; 9(10): 849-849.
- Alaggio R, Amador C, Anagnostopoulos I, Attygalle AD, Araujo IB de O, et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia. 2022; 36(7): 1720-48.
- Milette F. Review: Skin Lymphoma. The Illustrated Guide, 4th edition, by Lorenzo Cerroni. Dermatol Pract Concept. 2019.
- Vural S, Akay BN, Botsali A, Atilla E, Parlak N, et al. Transformation of Mycosis Fungoides/Sezary Syndrome: Clinical Characteristics and Prognosis. Turk J Hematol. 2018; 35(1): 35-41.
- Liu W, Yang Y, Qi S, Wang Y, He X, et al. Treatment, Survival, and Prognosis of Advanced-Stage Natural Killer/T-Cell Lymphoma: An Analysis From the China Lymphoma Collaborative Group. Front Oncol. 2021; 10.
- Ham MF, Ko YH. Natural killer cell neoplasm: biology and pathology. Int J Hematol. 2010; 92(5): 681-9.
- Chuang SS. In situ hybridisation for Epstein-Barr virus as a differential diagnostic tool for T- and natural killer/T-cell lymphomas in non-immunocompromised patients. Pathology (Phila). 2014; 46(7): 581-91.
- Sitthinamsuwan P, Pongpruttipan T, Bunyaratavej S, Karoopongse E, Kummalue T, et al. Cutaneous involvement by colonic extranodal NK/T-cell lymphoma mimicking mycosis fungoides: a case report. J Cutan Pathol. 2011; 38(12): 1004-8.
- Yu WW, Hsieh PP, Chuang SS. Cutaneous EBV-positive γδ T-cell lymphoma vs. extranodal NK/T-cell lymphoma: A case report and literature review. J Cutan Pathol. 2013; 40(3): 310-6.
- Pan ST, Chang WS, Murphy M, Martinez A, Chuang SS. Cutaneous Peripheral T-Cell Lymphoma of Cytotoxic Phenotype Mimicking Extranodal NK/T-Cell Lymphoma. Am J Dermatopathol. 2011; 33(2): e17-20.
- Feng Y, Rao H, Lei Y, Huang Y, Wang F, et al. CD30 expression in extranodal natural killer/T-cell lymphoma, nasal type among 622 cases of mature T-cell and natural killer-cell lymphoma at a single institution in South China. Chin J Cancer. 2017; 36(1): 43.
- Jawed SI, Myskowski PL, Horwitz S, Moskowitz A, Querfeld C. Primary cutaneous T-cell lymphoma (mycosis fungoides and Sézary syndrome). J Am Acad Dermatol. 2014; 70(2): 205.e1-205.e16.
- Scarisbrick JJ, Quaglino P, Prince HM, Papadavid E, Hodak E, et al. The PROCLIPI international registry of early‐stage mycosis fungoides identifies substantial diagnostic delay in most patients. Br J Dermatol. 2019; 181(2): 350-7.
- Shaum K, Aycock J. Cutaneous T-Cell Lymphoma with Nasal Necrosis. Arch Plast Surg. 2015; 42(02): 259-61.
- Arafah M, Zaidi SN, Kfoury HK, Al Rikabi A, Al Ghamdi K. The Histological Spectrum of Early Mycosis Fungoides: A Study of 58 Saudi Arab patients. Oman Med J. 2012; 27(2): 134-9.
- Jawed SI, Myskowski PL, Horwitz S, Moskowitz A, Querfeld C. Primary cutaneous T-cell lymphoma (mycosis fungoides and Sézary syndrome). J Am Acad Dermatol. 2014; 70(2): 223.e1-223.e17.
- NCCN. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ®) Primary Cutaneous Lymphomas. 2023.
- Latzka J, Assaf C, Bagot M, Cozzio A, Dummer R, et al. EORTC consensus recommendations for the treatment of mycosis fungoides/Sézary syndrome - Update 2023. Eur J Cancer. 2023; 195: 113343.
- Quaglino P, Prince HM, Cowan R, Vermeer M, Papadavid E, et al. Treatment of early-stage mycosis fungoides: results from the PROspective Cutaneous Lymphoma International Prognostic Index (PROCLIPI) study. Br J Dermatol. 2021; 184(4): 722-30.
- Phan K, Ramachandran V, Fassihi H, Sebaratnam DF. Comparison of Narrowband UV-B with Psoralen-UV-A Phototherapy for Patients with Early-Stage Mycosis Fungoides. JAMA Dermatol. 2019; 155(3): 335.
- Grandi V, Simontacchi G, Grassi T, Pileri A, Pimpinelli N. Short‐term efficacy and safety of total skin electron beam therapy in mycosis fungoides: Systematic review and meta‐analysis. Dermatol Ther. 2022; 35(11).
- Hristov AC, Tejasvi T, A Wilcox R. Cutaneous T-cell lymphomas: 2021 update on diagnosis, risk-stratification, and management. Am J Hematol. 2021; 96(10): 1313-28.
- Semaan S, Abel MK, Raffi J, Murase JE. A clinician’s guide to cutaneous T-cell lymphoma presenting as recalcitrant eczematous dermatitis in adults. Int J Womens Dermatol. 2021; 7(4): 422-7.
- Miyagaki T. Diagnosis of Early Mycosis Fungoides. Diagnostics. 2021; 11(9): 1721.
- Lee H. Mycosis fungoides and Sézary syndrome. Blood Res. 2023; 58(S1): S66-82.
- Tanaka H, Mori E, Akutsu T, Saito S, Tei M, et al. Characteristics of Extranodal NK/T-Cell Lymphoma, Nasal Type, Compared with Nasal Diffuse Large B-cell Lymphoma. Clin Med Insights Oncol. 2023; 17: 117955492311566.
- Qin L, Li Y, He Y, Zeng R, Pan T, et al. Successful Treatment of Primary CNS Extranodal NK/T-Cell Lymphoma with Surgery and Chemotherapy Combined with Sintilimab: A Case Report and Literature Review. Onco Targets Ther. 2022; 15: 1-11.
- Parida DK, Barik SK. Surviving With Mycosis Fungoides for Twenty Years: An Autobiographical Case Report. Cureus. 2021.
- Yan J, Liu W, Wang X, Zhao S, Gao L, et al. Primary Central Nervous System Extranodal Natural Killer/T-Cell Lymphoma, Nasal Type Colliding with Meningioma. World Neurosurg. 2018; 120: 17-26.
- Hong M, Lee T, Young Kang S, Kim SJ, Kim W, et al. Nasal-type NK/T-cell lymphomas are more frequently T rather than NK lineage based on T-cell receptor gene, RNA, and protein studies: lineage does not predict clinical behavior. Mod Pathol. 2016; 29(5): 430-43.
- Zhao Q, Fan S, Chang Y, Liu X, Li W, et al. Clinical efficacy of cisplatin, dexamethasone, gemcitabine and pegaspargase (DDGP) in the initial treatment of advanced stage (stage III-IV) extranodal NK/T-cell lymphoma, and its correlation with Epstein-Barr virus. Cancer Manag Res. 2019; 11: 3555-64.
