
Open Access, Volume 10
An anterior mediastinal cystic tuberculoma mimicking echinococcosis
Caterina Di Ceccoa; Jacopo Monticellia*
Infectious Diseases Unit, Trieste University Hospital (ASUGI), Piazza dell’Ospitale 1, 34129 - Trieste, Italy.
Jacopo Monticelli
Infectious Diseases Unit, Trieste University Hospital (ASUGI), Piazza dell’Ospitale 1, 34129 - Trieste, Italy.
Tel: +39-0403992594 &+39-0403992652;
Email: jacopo.monticelli@asugi.sanita.fvg.it
Received : August 29, 2024,
Accepted : September 20, 2024
Published : September 27, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Tuberculosis is recognized as a “great imitator” and certain atypical presentations may be misdiagnosed as other diseases. Only a limited number of cases of isolated anterior mediastinal tuberculosis have been documented in the literature, particularly among immunocompetent patients. We present the case of a 65-year-old immunocompetent man from Southern Italy with a history of congenital heart disease corrected surgically in childhood, who presented with a large retrosternal cystic collection initially suspected to be an echinococcal cyst, subsequently diagnosed as a tuberculoma.
Keywords: Tuberculosis; Mediastinum; Echinococcosis; Cyst.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Monticelli J (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Ceccoa CD, Monticellia J. An anterior mediastinal cystic tuberculoma mimicking echinococcosis. Open J Clin Med Case Rep. 2024; 2287.
Introduction
Tuberculosis, caused by Mycobacterium tuberculosis complex, and cystic echinococcosis, caused by Echinococcus granulosus, are both rare endemic infections in Italy. In 2020, the incidence of tuberculosis in Italy reported by the European Centre for Disease Prevention (ECDC) was 6.6 per 100,000 people/year [1] and, despite the absence of a national surveillance system for echinococcosis, the annual human incidence of cystic echinococcosis has been reported as high as 6.41 per 100,000/year people in some regions of Southern and Insular Italy, particularly in Sicily, Sardinia and Basilicata [2]. Extrapulmonary tuberculosis in Italy represents less than 30% of reported cases of tuberculosis [1] and while mediastinal tuberculosis is commonly associated with tubercular lymphadenopathy, tuberculoma- intended as an isolated collection of tubercles potentially mimicking a mass- is even rarer, especially in the anterior mediastinum compartment.
The differential diagnosis of anterior mediastinal masses is very broad and includes neoplasms (such as liposarcoma, thymolipoma, teratoma, lymphoma, germ cell tumors, etc.), thyroid goiter, vascular aneurysms, sarcoidosis, silicosis, bacterial abscesses, pleural or pericardial cysts. Computerized Tomography (CT) attenuation values help the clinician to narrow the spectrum of causes but the etiological gold standard is the histological examination via biopsy or surgery [3]. Only few cases of isolated anterior mediastinal tuberculosis are reported in the English medical literature, especially in adult immunocompetent patients [4-11]. Tuberculosis is known as a “great imitator” and, while it is becoming increasingly less prevalent in Europe and Italy, some uncommon manifestation of tuberculosis might be misdiagnosed with other diseases, albeit rare ones such as cystic echinococcosis.
Case Presentation
We present the case of a 62-year-old man from Messina (Sicily, Italy) with a medical history of congenital subvalvular aortic stenosis surgically repaired in 1973. The patient resides in an urban setting, owns a pet dog, and denied any past or recent contact with farm animals. He reported occasional trips to Romania and denied any past or recent close contact with tuberculosis cases. Notably, a relative had a history of echinococcosis (splenic cyst) and died from unrelated causes.
In March 2022, after a paucisymptomatic SARS-CoV-2 infection, he started to complain of fever and dyspnea. A contrast-enhanced chest Computerized Tomography (CT) scan revealed a retrosternal cystic collection (72 x 53 mm) with associated peripheral calcifications, initially interpreted as outcomes of pericarditis. A 18F-fluorodeoxyglucose positron emission tomography scan (June 2022) confirmed the presence of the antero-inferior mediastinal lesion characterized by a low uptake of tracer and hyperactive rim (standardized uptake value: 9.7 on hepatic mean of 4.3).
In October 2022 he was admitted to the cardiology department of our hospital (Trieste, Friuli-Venezia Giulia, Italy) for congestive heart failure (New York Heart Association classes: III-IV), secondary to ab extrinsic compression by the mediastinal formation. A cardiac Magnetic Resonance Imaging (MRI) demonstrated the dimensional increase of the known retro-xiphoid collection (8 x 5 x 7 cm) with fluid content and rim enhancement. A contrast-enhanced transesophageal echocardiography characterized the lesion as an anechoic oval structure without rim capture, displaying areas of solid appearance and increased echogenicity internally. Considering all findings, the imaging suggested a collection consistent with an infectious etiology.
Among the results of the investigations carried out, the following are worth mentioning: Echinococcus IgG serology (by chemiluminescence immunoassay method) resulted negative; nucleic acid amplification for Entamoeba histolytica/dispar on feces resulted negative; QuantiFERON-TB Gold Plus (QFT®-Plus; Qiagen) resulted positive, suggesting a tubercular infection (at least a latent infection). A contrast-enhanced chest CT scan ruled out pulmonary parenchymal involvement but revealed extension of the mediastinal collection both above and below the diaphragm, with contact noted with both the pericardium and the hepatic capsule. Notably, the cyst capsule did not show ring enhancement after contrast, as was expected by a collection of infectious origin (Figure 1). Moreover, the chest CT showed numerous calcifications in the pericardial area (Figure 2). Following multidisciplinary discussion, on November 16, 2022, the patient underwent surgery for the removal of the cystic formation. Intraoperative samples revealed acid-fast bacilli, identified by nucleic acid amplification (Xpert® MTB/RIF; Cepheid) as rifampin-susceptible M. tuberculosis complex, subsequently confirmed by traditional mycobacterial culture to be pan-susceptible M. tuberculosis. Sputum and bronchial aspiration cultures were negative for acid-fast bacilli. Based on the findings from the intraoperative samples, antitubercular therapy was started using a standard intensive phase regimen (rifampin 10 mg/kg/day, isoniazid 5 mg/kg/day, pyrazinamide 25 mg/kg/day, ethambutol 20 mg/kg/day).
After a few weeks, treatment was discontinued due to the development of iatrogenic hepatitis. Upon normalization of hepatocellular injury markers, therapy was gradually resumed and continued with the standard intensive regimen for two months, followed by isoniazid and rifampin for an additional ten months (until February 2024) in another city hospital near his hometown (Catania, Sicily, Italy). Follow-up radiological examinations (chest CT scan and cardiac MRI) conducted during therapy demonstrated a post-operative fluid collection in the area of excised cyst, although with reduced volume and minor clinical impact. Until our most recent telephone follow-up evaluation (May 21, 2024), the patient remained in good clinical condition.
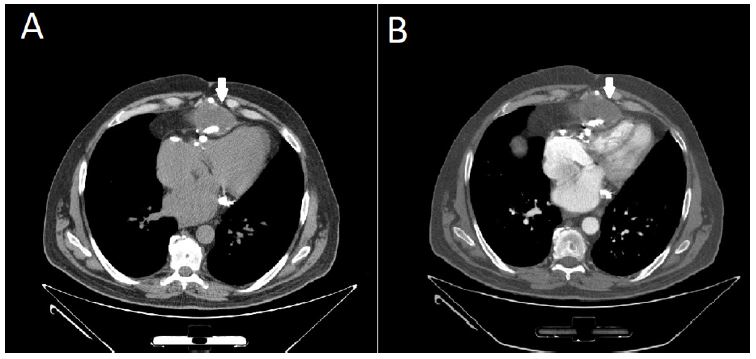
Figure 1: Axial chest CT scans before (A) and after (B) contrast enhancement. The cyst capsule (marked with a white arrow) do not show ring enhancement after contrast.
Figure 2: Sagittal chest CT scan. The cyst capsule is marked with a white arrow. Numerous calcifications are visible in the pericardial area.
Discussion
Considering the variety of different tissues in the anterior mediastinum, it is not surprising that the differential diagnosis of anterior mediastinal masses is very broad. Mediastinal masses tend to manifest themself in a variety of different symptoms (due to the compression of local structures) ranging from chest pain, cough and dyspnea [8]. In the case of our patient, his mediastinal mass manifested at the onset with fever and dyspnea due to a congestive heart failure secondary to ab extrinsic compression. At the beginning, our patient’s mass imaging characteristics and the slowly progressive worsening of the initial symptoms suggested an etiology by a subacute or chronic infection, however the spectrum of potential infective agents was broad. In Sicily, our patient’s home region, echinococcosis and tuberculosis are both uncommon diseases with comparable incidence (around 6.5 per 100,000 people/year). In the initial diagnostic work-up, the MRI and echocardiographic findings suggested a potential cystic echinococcosis. Cystic echinococcosis (caused by E. granulosus) is distinguished by alveolar echinococcosis (caused by E. multilocularis) by the formation of frequently isolate cysts in the liver, but lung involvement is not uncommon (20% of cases) [12]. However, primary anterior mediastinal echinococcosis is extremely rare [13] but the “hourglass” transdiaphragmatic CT appearance of the patient’s mediastinal cyst might have suggested a migration from a contiguous hepatic cyst. Echinococcus serology resulted negative. This result reduced the pre-surgical possibility of diagnosis of echinococcosis and, in fact, M. tuberculosis was found in the intra-operative samples. Mediastinal tuberculosis is also a rare etiology in the differential diagnosis of anterior mediastinal lesions. Tubercular involvement of mediastinal structures consists mainly in solid or partially colliquated hilar lymphadenopathy or a collection of caseum originating from bronchial or pulmonary or pleural or lymphatic lesions. As described elsewhere, Cystic anterior mediastinal tuberculosis is extremely rare, especially in immunocompetent hosts, with less than ten cases described in the English medical literature so far [4-11]. Moreover, tuberculosis rarely manifests with cystic lesions, and in those rare cases, cysts are multiple and limited to the lung parenchyma [14]. In our patient, complete exeresis of the cystic lesion, followed by 12 months of standard regimen of antitubercular drugs, was considered the best therapeutic option.
Conclusion
In conclusion, both tuberculosis and cystic echinococcosis are rare etiology of anterior mediastinal masses but we suggest to maintain a high clinical suspicion. We also suggest that microbiological and histological examination of resected masses are pivotal in the definitive diagnosis and subsequent management of these infrequent mediastinal infections.
References
- European Centre for Disease Prevention and Control, WHO Regional Office for Europe. Tuberculosis surveillance and monitoring in Europe 2022- 2020 data. [https://www.ecdc.europa.eu/sites/default/files/documents/Tuberculosis-surveillance-monitoring-europe-2022_0.pdf. Last accessed 23th of April 2023.]
- Entezami M, Nocerino M, Widdicombe J, Bosco A, Cringoli G, et al. The spatial distribution of cystic echinococcosis in Italian ruminant farms from routine surveillance data. Front. Trop. Dis. 2022; 3: 1034572.
- Shahrzad M, Le TS, Silva M, Bankier AA, Eisenberg RL. Anterior mediastinal masses. AJR Am J Roentgenol. 2014; 203(2): W128-38.
- Butler J, Barry S. Rare case of cystic anterior mediastinal tuberculosis in an immunocompetent patient. Respirol Case Rep. 2022; 10(7): e0987.
- Maguire S, Chotirmall SH, Parihar V, Cormican L, Ryan C, et al. Isolated anterior mediastinal tuberculosis in an immunocompetent patient. BMC Pulm Med. 2016; 16: 24.
- Khilnani GC, Jain N, Hadda V, Arava SK. Anterior mediastinal mass: A rare presentation of tuberculosis. J Trop Med. 2011; 2011: 635385.
- De Ugarte DA, Shapiro NL, Williams HL. Tuberculous mediastinal mass presenting with stridor in a 3-month-old child. J Pediatr Surg. 2003; 38(4): 624-625.
- Kumar N, Gera C, Philip N. Isolated mediastinal tuberculosis: A rare entity. J Assoc Physicians India. 2013; 61(3): 202-3.
- Vincken W, Vandenbrande P, Roels P, Pirngadi J, Welch W. Isolated paratracheal mass of tuberculous origin in an adult patient. Eur J Respir Dis. 1983; 64(8): 630-5.
- Sattavarapu LR, Narahari NK, Balaram DS, Kapoor A, Paramjyothi GK. An Unusual Cause of Mediastinal Mass and Chylothorax. Int J Appl Basic Med Res. 2020; 10(2): 143-146.
- Leye M, Jobe M, Diatta S, Ndiaye MB, Aw F, et al. A case of pericardial tuberculoma presenting as a left anterior chest wall mass. Int Arch Med. 2013; 6(1): 48.
- Brunetti E, Kern P, Vuitton DA. Writing Panel for the WHO-IWGE. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop. 2010; 114(1): 1-16.
- Rakower J, Milwidsky H. Primary mediastinal echinococcosis. Am J Med. 1960; 29: 73-83.
- Van LD, Le HN, Pletschette M, Nguyen AT, Nguyen TH, et al. Cystic pulmonary tuberculosis: A rare form of an ancient disease. Respirol Case Rep. 2022; 10(9): e01020.
