
Open Access, Volume 10
Organ morphogenesis proteins contribution in colorectal cancer
Monika Kozlowska-Geller*; Piotr Lewitowicz; Agnieszka Strzelecka; Lukasz Nawacki; Justyna Klusek; Monika Wawszczak-Kasza; Stanislaw Gluszek
Collegium Medicum, The Jan Kochanowski University in Kielce, Poland.
Monika Kozlowska-Geller
Collegium Medicum, Aleja IX Wieków Kielc 19A, 25-317 Kielce, Poland.
Email: monika.kozlowska-geller@ujk.edu.pl
Received : August 21, 2024,
Accepted : September 17, 2024
Published : September 27, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Introduction: Colorectal Cancer (CRC) is the third most common cancer worldwide, with 1-2 million new cases diagnosed annually and the fourth leading cause of cancer-related deaths. Transcription factors involved in embryogenesis and organ morphogenesis play also an important role as the triggers and modulators of carcinogenesis. Their overactivity promotes cancer cell proliferation, migration, epithelial-mesenchymal transition, and finally invasion.
Aim: This study aimed to assess FOXA-1, FOXP–1, EZH-2, and INI-1 expression in colon cancer in aspect patient age, clinical outcome, and approved predictors.
Material and methods: One hundred thirteen patients with stage II-IV CRC who underwent surgery due to CRC between 2005-2011 were included to the study. We tabularized all requested clinical data and performed immunohistochemical analysis of FOXA1, FOXP1, EZH-1, INI-1.
Results: According to the patients’ age we observed higher incidence of FOXA-1 (p=0.01) and the coexistence of FOXA-1/FOXP-1 (p=0.027) in people over 55 years of age. Cox regression model did not reveal FOX expression in Overall Survival (OS) (p>0,05). Our observations confirmed the well-documented value of TNM (HR=0,02; p=0,001) and patient age in prognosis (HR=0,44; p=0,01). A statistically significant relationship was found between the coexistence of certain factors: FOXA-1 and FOXP-1 (OR=17,90; p=0,000), INI-1 (OR=3,90; p=0,002).
Conclusion: All studied proteins contribute in CRC.
Keywords: Colorectal cancer; Case; Cancer; Cell; Patient.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Kozlowska-Geller M (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Kozlowska-Geller M, Lewitowicz P, Strzelecka A, Nawacki L, Klusek J, Wawszczak-Kasza M, Gluszek S. Organ morphogenesis proteins contribution in colorectal cancer. Open J Clin Med Case Rep. 2024; 2285.
Introduction
Colorectal Cancer (CRC) is the third most common cancer worldwide, with 1-2 million new cases diagnosed annually, and the fourth leading cause of cancer-related deaths, with 700,000 death reported every year [1]. Transcription factors play important roles in the pathogenesis of colorectal cancer. They often contribute to carcinogenesis in various stages. Therefore, they may have predictive value as biomarkers [2].
The development of specific and more sensitive biomarkers will improve the diagnosis and enable the detection of CRC in the earliest stages of the disease, thus improving prognosis. Therefore, various panels of biomarkers are being developed to improve prognosis and select the appropriate treatment [3].
Forkhead box protein A1 (FOXA1), a founding member of the FOX family of transcription factors, is involved in CRC progression. FOXA1 can bind to the promoters of more than 100 genes to influence signaling pathways and the cell cycle in human cancers [4,5]. Foxp1 is a tumor suppressor in colon cancer [6]. The Forkhead Box 1 (Foxp1) protein is part of the P subfamily of the Forkhead Box (FOX) family. These proteins affect embryo development, regulate the cell cycle, and participate in metabolism and immune regulation. Disorders in gene expression of these proteins may be associated with carcinogenesis [7,8].
Enhancer of zeste homolog 2 (EZH2) is associated with epigenetic gene silencing and aggressiveness in many tumor types [9]. EZH2 is also involved in metastasis by modulating tumor angiogenesis and epithelial-to-mesenchymal transition, a process by which disseminating tumor cells acquire mesenchymal characteristics to migrate through the extracellular matrix [6].
SMARCB1 is a tumor suppressor gene that encodes INI1. Interactions have been demonstrated between SMARCB1/INI1 and key proteins in various pathways related to tumor proliferation and progression, including the p16-RB pathway, WNT signaling pathway, sonic hedgehog signaling pathway, and Polycomb pathway [7].
The increase in IGF-1R activity promotes carcinogenesis and tumor aggression and is associated with metastases, treatment resistance, poor prognosis and shorter survival [8].
The objective of the study
The objective of this study was to assess FOXA -1, FOXP-1, EZH-2, INI-1, and IGF-1R immunoreactivity in colon cancer especially in patients up to 55 years of age and to determine the clinical outcome.
Material and Methods
The research was carried out in the Department of Clinical and Experimental Pathology of the Jan Kochanowski University in Kielce, the Holy Cross Cancer Center and in the Clinic of General, Oncological and Endocrine Surgery of the Provincial Hospital in Kielce.
Study patients
Using the appropriate criteria, we qualified 113 women and men with primary adenocarcinoma in stages II-IV, who had been operated on between 2005-2011, due to colorectal cancer, for the study. They did not have other gastrointestinal tract tumors, and all patients who received adjuvant pre-operative radiotherapy were excluded. These patients had no medical condition (internal, cardiological, or pulmonary). The clinical outcomes were Overall Survival (OS) and 17th years follow up.
Research methodology
The research methodology consisted of two steps. First step, we retrospectively analyzed the medical histories of patients who qualified for the study.
After obtaining written consent, 113 patients with colorectal cancer confirmed by histopathological examination, aged 32-87, were included in the study (46 women and 67 men). The follow-up studies covered a period of 17 years.
Immunohistochemical tests
Classic immunohistochemical tests were performed using anti-FOXA-1 (2F83), anti-FOXP-1(SP133), anti-EZH2 (SP129), anti-INI-1(MRQ-27), and anti-IGF-1R (G11) antibodies. All the tests performed had been fully validated with the intention of using in vitro. All reactions were performed using BenchMark XT (Ventana Medical Systems; Roche Group, Tucson, USA). After a fully automated dewaxing and repeated hydration reaction of the samples, unmasking of the antigen by proteinase K (37°C, 5 min) was conducted, followed by incubation with the primary antibodies (1:50 dilution, 20 min incubation). The time and temperature of antigen retrieval and incubation with primary antibodies were strictly in accordance with the manufacturer’s recommendations, followed by further routine steps. A universal DAB Ventana Detection it was used. A two-level scale describing factor reactivity was used: 0 - no reaction (negative); 1- strong reaction (positive).
Digital and statistical analysis
All calculations were performed using digital slide analysis with a Hamammatsu NanoZoomer S210 slide scanner (Hamamatsu®, Hamamatsu City, Shizuoka Pref. Japan). After scanning the entire slide, digital image analysis was performed using the Visiopharm membrane application (Visiopharm®, Hoersholm, Denmark). The application allowed us to diversify the intensity of the plasmalemmal reaction and avoid subjectivity. The collected data were subjected to statistical analysis using the Kaplan-Meier method, log-rank test, Cox proportional hazard model, rho Spearman test and logistic regression. In the tests, a significance level of 0,05 was adopted for the purposes of statistical inference. Licensed SAS 9.3 software and Excel were used for the statistical analyses.
Results
Clinicopathological data and survival analysis
The clinical observation period was 17 years. The clinical outcome was Overall Survival (OS). Among the 113 patients examined, 44 were aged than or equal to 55 years. 63 survived until the end of 5 years (56%), 50 patients (44%) did not survive, and the median survival was 26 months. Among patients less than or equal to 55 years of age, 13 people did not survive, and their median survival was 26 months. Among patients aged >55 years, 35 did not survive, and their median survival was 26 months.
Relationship between factors immunoexpression and clinical-pathological features
Age: The frequency of the factors in the patients under observation varied according to age. FOXA-1 proteins (p=0.01) and a combination of FOXA-1 and FOXP-1 proteins (p=0.027) were significantly more common in the elderly (over 55 years of age). The frequency of EZH-2 (p=0.446), INI-1 (p=0.368) and IGF-IR (p=0.276) proteins did not differ significantly by age (Table 1).
Overall survival: The distributions of Overall Survival (OS) in patients with immunoexpression of the tested factors and in those without expression differed insignificantly (p< 0.05) (Table 2).
Table 1: Frequency of occurrence of individual proteins depending on the age of the examined patients.
| Occurance | Age<=55 lat (n=44;%) | Age>55 lat (n=69;%) | Together (n=113; %) | p-value* |
|---|---|---|---|---|
| FOXP-1 positiveNo | 11(25.00) | 26(37.68) | 37(32.74) | 0. 161 |
| FOXA-1 | ||||
| Yes No | 11(25.00)33(75.00) | 39(56.52)30(43.48) | 50(44.25)63(55.75) | 0.001* |
| FOXP-1 and FOXA-1 | ||||
| Yes No | 8(18.18)36(81.82) | 26(37.68)43(62.52) | 34(30.09)79(69.91) | 0.027* |
| EZH-2 | ||||
| Yes No | 23(52.27)21(47.73) | 31(44.93)38(55.07) | 54(47.79)59(52.21) | 0.446 |
| INI-1 | ||||
| Yes No | 16(36.36)28(63.64) | 31(44.93)38(55.07) | 47(41.59)66(58.41) | 0.368 |
| IGF-1R | ||||
| Yes No | 30(68.18)14(31.82) | 40(57.97)29(42.03) | 70(61.95)43(38.05) | 0.276 |
*χ2 test, **p< α; α=0,05, statistical significance
Table 2: Overall Survival (OS) and the occurence of individual factors in the examined patients.
| Type of factors | n | Me | IQR | Min | Max | P-value* |
|---|---|---|---|---|---|---|
| FOXP-1 Yes | 37 | 2.00 | 5.00 | 0.00 | 16.00 | 0.210 |
| FOXP-1 No | 76 | 2.50 | 7.50 | 0.00 | 18.00 | |
| FOXA-1 Yes | 50 | 2.00 | 4.00 | 0.00 | 16.00 | 0.081 |
| FOXA-1 No | 63 | 3.00 | 9.00 | 0.00 | 18.00 | |
| FOXP-1& FOXA-1 Yes | 34 | 2.50 | 5.00 | 0.00 | 16.00 | 0.491 |
| FOXP-1& FOXA-1 No | 79 | 2.00 | 7.00 | 0.00 | 18.00 | |
| EZH-2 Yes | 54 | 2.50 | 7.00 | 0.00 | 18.00 | 0.875 |
| EZH-2 No | 59 | 2.00 | 7.00 | 0.00 | 18.00 | |
| INI-1 Yes | 47 | 2.00 | 5.00 | 0.00 | 18.00 | 0,223 |
| INI-1 No | 66 | 2.50 | 8.00 | 0.00 | 18.00 | |
| IGF-1R Yes | 70 | 0.00 | 7.00 | 0.00 | 18.00 | 0,295 |
| IGF-1R No | 42 | 3.00 | 7.00 | 0.00 | 18.00 |
ATest U Manna-Whitneya p>α; α=0.05, Me: Median, IQR: Interquartile range
Table 3: Final predictors included in the (logistic regression) model of FOXP-1, of FOXA-1, for INI for IGF-1R.
| Variable | Estimate of the logistic regression parameter | OR(95% Cl) | p-value |
|---|---|---|---|
| Final predictors included in the (logistic regression) model of FOXP-1 | |||
| Constant term | -3.818 | 0.022(0.005-0.090) | 0.000 |
| FOXA-1 | 2,956 | 19.221(4.777-77.347) | 0.000 |
| INI-1 | 2,342 | 10.401(2.988-36.208) | 0.000 |
| Final predictors included in the(logistic regression) modelof FOXA-1 | |||
| Constant term | -2.584 | 0.075(0.025-0.228) | 0.000 |
| FOXP-1 | 2.885 | 17.903(4.228-75.812) | 0.000 |
| INI-1 | 1.360 | 3.896(1.219-12.454) | 0.022 |
| IGF-1R | 1.430 | 4.179(1.258-13.880) | 0.020 |
| Final predictors included in the (logistic regression) model for INI | |||
| Constant term | -2.140 | 0.118(0.042-0.332) | 0.000 |
| FOXA-1 | 2.140 | 8.500(2.042-35.381) | 0.003 |
| FOXP-1 | 1.569 | 4.800(1.214-18.972) | 0.025 |
| Final predictors included in the(logistic regression) modelfor IGF-1R | |||
| Constant term | -1.310 | 0.270(0.123-0.592) | 0.001 |
| EZH-2 | 2.128 | 8.398(2.175-32.429) | 0.002 |
| FOXA-1 | 1.570 | 4.806(1.418-16.284) | 0.012 |
Death
• The presence of the analyzed factors does not affect the risk of deFOXP-1 HR 0,86; 95% CI: 0,48-1,54; p= 0,624.
• FOXA-1 HR 0,86; 95% CI: 0,49-1,50; p=0,594
• FOXP-1 and FOXA-1 HR 1,00; 95% CI: 0,55-1,84; p=0,989
• EZH-2 HR 1,00; 95% CI: 0,57-1,1,73; p=0,989
• INI HR 0,91; 95% CI: 0,52-1,54; p=0,730
• IGF-1R HR 0,63; 95% CI: 0,34-1,17; p=0,147
Relationships between the observed variables
The increase in FOXP-1 expression was accompanied over 19 times higher expression of FOXA-1 (OR=19.221; 95% Cl: 4.777-77.347; p 0.000) and over 10 times higher expression of INI-1 (OR=10.401; 95% Cl: 42.988-36.208; p=0.000) (Table 3).
The value of the statistic HS=2.6057, with a value of p=0.106, indicated a significant fit of the logistic regression model. Based on the analysis of the area under the ROC curve, one can also state that the model fits the data well (the Area Under the Curve (AUC) is 0.917) and is characterized by a good predictive ability resulting from the obtained sensitivity and specificity graphs for different levels of probability (Figure 1).
The increase in FOXA-1 expression was accompanied almost 18 times the expression of FOXP-1 (OR=17.903; 95% Cl: 4.228-75.812; p 0.000), four times that of INI-1 (OR=3.896; 95% Cl: 1.219-12.454; p 0.022) and IGF-1R (OR=4.179; 95% Cl: 1.258-13.880; p=0.020) (Table 3).
The value of the statistic HS=1.1325, with at value of p=0.568, indicated a significant fit of the logistic regression model. Based on the analysis of the area under the ROC curve, one can also state that the model fits the data well (the Area Under the Curve (AUC) is 0.900) and is characterized by a good predictive ability resulting from the obtained sensitivity and specificity graphs for different levels of probability (Figure 2).
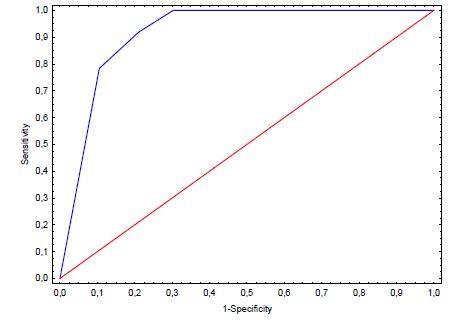
Figure 1: The ROC curve graph for FOXP-1.
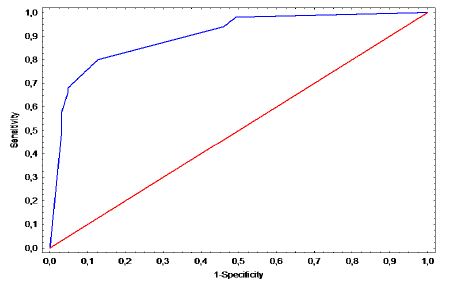
Figure 2: The ROC curve graph for FOXA-1.
Table 4: elationship between INI-1 expression and IGF-1R expression observed variables (total age up to 55 years and over 55 years).
| Correlations betweenINI-1 expression and observed variables | rho Spearman | p-value* | rho Spearman | p-value* | rhoSpearman | p-value* |
|---|---|---|---|---|---|---|
| Total (n=113) | Age up to 55(n=44) | Ageover 55 (n=69) | ||||
| TNM | 0.123 | 0.196 | 0,283 | 0,063 | 0,027 | 0,826 |
| FOXP-1 | 0.636 | 0.000** | 0,764 | 0,000** | 0,560 | 0,000** |
| EZH-2 | 0.523 | 0.000** | 0,533 | 0,000** | 0,531 | 0,000** |
| FOXA-1 | 0.586 | 0.000** | 0,655 | 0,000** | 0,557 | 0,000** |
| FOXA-1 and FOXP-1 | 0.582 | 0.000** | 0,624 | 0,000** | 0,560 | 0,000** |
| STANDARD WEIGHT | -0.060 | 0.525 | -0,163 | 0,291 | -0,061 | 0,620 |
| OVERWEIGHT | 0.093 | 0.326 | -0,017 | 0,913 | 0,103 | 0,400 |
| 1st degree OBESITY | 0.032 | 0.736 | 0,176 | 0,253 | -0,052 | 0,670 |
| 2nd degree OBESITY | 0.023 | 0.810 | - | - | 0,018 | 0,886 |
| IGF-1R | 0.329 | 0.000** | 0,314 | 0,038** | 0,356 | 0,003** |
| Correlations between IGF-1R expression and and observedvariables | rho Spearman | p-value* | rho Spearman | p-value* | rho Spearman | p-value* |
| Total (n=113) | Age up to 55(n=44) | Age over 55(n=69) | ||||
| TNM | 0.161 | 0.089 | 0.314 | 0.038** | 0.056 | 0.648 |
| FOXP-1 | 0.314 | 0.001** | 0.169 | 0.273 | 0.420 | 0.000** |
| EZH-2 | 0.458 | 0.000** | 0.324 | 0.032** | 0.533 | 0.000** |
| FOXA-1 | 0.405 | 0.000** | 0.282 | 0.064 | 0.556 | 0.000** |
| FOXA-1&FOXP-1 | 0.315 | 0.001** | 0.196 | 0.203 | 0.420 | 0.000** |
| STANDARD WEIGHT | -0.106 | 0.265 | -0.297 | 0.050 | 0.011 | 0.927 |
| OVERWEIGHT | -0.005 | 0.961 | -0.009 | 0.955 | 0.042 | 0.735 |
| 1st degree OBESITY | -0.019 | 0.845 | -0.063 | 0.685 | 0.022 | 0.860 |
| 2nd degree OBESITY | -0.171 | 0.070 | - | - | -0.203 | 0.094 |
| INI-1 | 0.329 | 0.000** | 0.314 | 0.038** | 0.356 | 0.003** |
* Spearman rank correlation coefficient, **p< α, α=0,05
A relationship was observed between INI-1 expression and FOXP-1 (r=0.636, p=0.000), EZH-2 (r=0.523, p=0.000), FOXA-1 (r=0.586, p=0.000) and IGF-1R (r=0.329, p=0.000). There was no higher INI-1 expression in overweight and obese (BMI) patients. Age did not determine the differences in the relationships between the analyzed variables (Table 4).
The above relationships were confirmed in the logistic regression model, where the increase in INI expression was accompanied by 8,5 times higher expression of FOXA-1 (OR=8.500; 95% Cl: 2.042-35.381; p 0.003), and almost 5 times higher expression of FOXP-1 (OR=4.800; 95% cl: 1.214-18.972; p=0.025) (Table 3).
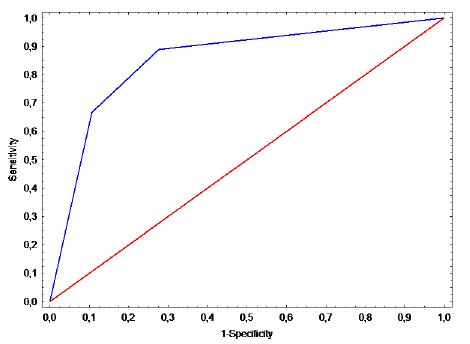
Figure 3: The ROC curve for INI.
The value of the statistic HS=1.978, with at value of p=0.168, indicated a significant fit of the logistic regression model. Based on the analysis of the area under the ROC curve, one can also state that the model fits the data well (the Area Under the Curve (AUC) is 0.851) and is characterized by a good predictive ability resulting from the obtained sensitivity and specificity graphs for different levels of probability (Figure 3).
A relationship was observed between IGF-1R expression and FOXP-1 (r=0.314, p=0.001), EZH-2 (r=0.458, p=0.000), FOXA-1 (r=0.405, p=0.000), and INI-1 (r=0.329, p=0.001). There was no higher IGF-1R expression in overweight or obese (BMI) patients. Age determined the relationships between the analyzed variables - in patients aged up to 50 years, only a correlation was found between IGF-1R expression and TNM (r=0.314, 0=0.038) EZH-2 (r=0.324, 0.032) and INI-1 (r=0.314, p=0.038) (Table 4).
The above relationships were confirmed in the logistic regression model, where the increase in IGF-1R expression was accompanied by over 8 times higher expression of EZH-2 (OR=8.398; 95% Cl: 2.175-32.429; p=0.002) and almost 5 times higher expression of FOXA-1 (OR=4.806; 95% Cl: 1.418-16.284; p=0.012) (Table 3).
The value of the statistic HS=0.0260, with at value of p=0.872, indicated a significant model fit of the logistic regression model. Based on the analysis of the area under the ROC curve, one can also state that the model fits the data well (AUC=0.847) and is characterized by good predictive ability resulting from the obtained sensitivity and specificity graphs for different levels of probability (Figure 4).
In the group of patients up to 55 years of age, increased expression of FOXP-1 (r=0,321, p=0,034) and IGF-IR (r=0,314, p=0,038) was observed with increasing TNM stage (Table 5).
Table 5: Relationships between TNM and observed variables (total age up to 55 years and over 55 years).
| Correlations between TNM and observed variables | rho Spearman | p-value* | rho Spearman | p-value* | rho Spearman | p-value* |
|---|---|---|---|---|---|---|
| Total (n=113) | Age up to 55(n=44) | Ageover 55 (n=69) | ||||
| FOXP-1 | 0.144 | 0.129 | 0.321 | 0.034** | 0.040 | 0.747 |
| EZH-2 | 0.059 | 0.535 | 0.130 | 0.401 | 0.020 | 0.870 |
| FOXA-1 | 0.066 | 0.489 | 0.128 | 0.407 | 0.046 | 0.705 |
| FOXA-A&FOXA-P | 0.065 | 0.491 | 0.134 | 0.385 | 0.040 | 0.747 |
| STANDARD | -0.124 | 0.191 | -0.108 | 0.486 | -0.139 | 0.255 |
| OVERWEIGHT | -0.072 | 0.447 | -0.158 | 0.306 | -0.040 | 0.745 |
| 1st degreeOBESITY | 0.063 | 0.505 | -0.067 | 0.665 | 0.137 | 0.263 |
| 2nd degreeOBESITY | 0.135 | 0.153 | - | - | 0.185 | 0.128 |
| INI-1 | 0.123 | 0.196 | 0.283 | 0.063 | 0.027 | 0.826 |
| IGF-1R | 0.161 | 0.089 | 0.314 | 0.038** | 0.056 | 0.648 |
*Spearman rank correlation coefficient. **p< α. α=0.05
There were no predictors between the individual parameters. Only age determined this relationship. Among the young patients, up to 55. Significantly higher expression of FOXP-1 and FOXA-1 was observed with increasing BMI (r= 0.552, p=0.044) (Table 6).
Table 6: Relationship between BMI and observed variables (total age up to 55 years and over 55 years).
| Correlations between BMI and observed variables | rho Spearman | p-value* | rho Spearman | p-value* | rho Spearman | p-value* |
|---|---|---|---|---|---|---|
| Total (n=83) | Age up to 55(n=14) | Ageover 55 (n=69) | ||||
| FOXP-1 | 0.066 | 0.552 | 0.545 | 0.044** | -0.041 | 0.739 |
| EZH-2 | -0.082 | 0.462 | 0.000 | 1.000 | -0.101 | 0.410 |
| FOXA-1 | -0.050 | 0.652 | 0.579 | 0.030** | -0.199 | 0.100 |
| FOXA-A and FOXA-P | 0.066 | 0.552 | 0.545 | 0.044** | -0.041 | 0.739 |
| INI-1 | 0.111 | 0.317 | 0.355 | 0.213 | 0.054 | 0.657 |
| IGF-1R | -0.009 | 0.938 | 0.233 | 0.423 | -0.062 | 0.611 |
*Spearman rank correlation coefficient. **p<α. α=0.05
Discussion
Colorectal Cancer (CRC) is the third most common cancer and fourth most common cause of cancer-related deaths. The probability of colorectal cancer is approximately 4-5%. By 2030, the burden of CRC is expected to rise by 60% include 2,2 million new cases and 1,1 million CRC-related deaths [9]. With high morbidity and mortality worldwide, colorectal cancer is a global public health problem with high morbidity and mortality.
Transcription factors play an important role as trigger and modulators of carcinogenesis in many locations especially hormone-dependent malignancies. Overactivity promotes cancer cell proliferation, migration, and invasion. A biomarker is a biological entity used to detect a specific disease or monitor its progress and treatment effects [2,3].
The identification of new predictive and/or prognostic molecular biomarkers for CRC has become a priority for improving treatment outcomes [1,9].
In our study, we aimed to assess the expression of selected factors in patients with colorectal cancer, especially up to 55, and to detect relationships between these factors and clinicopathological features, including overall survival.
Forkhead box protein A1 (FOXA1), a founding member of the FOX family of transcription factors, participates in CRC progression. FOXA1 can bind to the promoters of more than 100 genes to influence signaling pathways and the cell cycle in human cancers, but its specific mechanism in CRC cells resistant to radiotherapy remains largely unknown [4,10].
Our study showed no relationship between increased FOXA-1 expression and poor survival (p=0,081). Similarly, FOXA-1 expression did not affect the risk of death (p=0,594). However, the increase in FOXA-1 expression was accompanied by almost 18 times higher expression of FOXP-1 and 4 times of INI-1and IGF-1R. Moreover, statistically significantly more often in the elderly (over 55 years of age) are FOXA-1 proteins (p=0.01), a combination of FOXA-1 and FOXP-1 proteins (p=0.027).
Little is known about the molecular mechanisms underlying Foxp1 loss in colon cancer. Foxp1 is a broadly expressed Foxp subset of “forkhead” (Fox) transcription factors [5,11,12]. Not surprising, that in our study the coexistence of FOXP-1 and other pathological factors has been demonstrated. Statistically significantly more often in the elderly (over 55 years of age) was a combination of FOXA-1 and FOXP-1 proteins (p=0.027). We observed, that the increase in FOXP-1 expression was accompanied by over 19 times higher expression of FOXA-1 and over 10 times higher expression of INI-1 (p=0,000).
Thus, it is not surprising that FOXP1 appears to play a role in malignancy. In our study, in the group of patients up to 55 years of age increased expression FOXP-1 (r=0,321, p=0,034) was observed with increasing TNM. The human genome contains 43 FOX genes. Many genes, including the four Foxp sub-family genes, are essential for development and organogenesis and generally function as transcriptional repressors [11,12]. The frequency of FOXP-1 proteins is not statistically significantly differentiated by age (p=0.276). In young patients up to 55years of age, significantly higher expression of FOXP-1 and FOXA-1 was found with increasing BMI (p=0,044).
To date, no follow-up studies have been published, on these findings in colon cancer or other gastrointestinal malignancies, and the impact of FOXP1 on survival and response to treatment remains to be determined [13].
Our studies showed no relationship between increased FOXP-1 expression and poor survival (p=0,210). Similarly, expression of FOXP-1 did not affect the risk of death: along (p=0,624) and FOXA-1 (p=0,989).
Currently available data are insufficient to conclusively determine whether FOXP1 functions as a tumor suppressor or as an oncogene, depending on the cell type, interacting partners, or subcellular localization. FOXP1 in a wide variety of cancers suggests that FOXP1 may be a therapeutic target or may be used to guide therapy [5,11].
The Enhancer of Zeste Homologue 2 (EZH2), a component of the polycomb repressive complex 2, is involved in stable transcriptional repression during embryogenesis and under pathological conditions such as cancer [6]. It is an important epigenetic regulator of genes that are involved in differentiation, proliferation, and stem cell renewal [14]. In cancer, it has been reported that EZH2 seems to play a dual role as either an oncogene or tumor suppressor; however, the molecular mechanisms underlying this antagonistic duality are not well understood, and the prognostic impact of high EZH2 expression is controversial for colorectal cancer [15].
The frequency of EZH-2 protein (p=0.446)was not significantly different by age. Our study showed no relationship between increased EZH2 expression and poor survival (p=0,875). Similarly, EZH2 expression did not affect the risk of death (p=0,989).
SMARCB1 is a tumor suppressor gene that encodes INI1. Loss of INI1 expression has recently been reported in gastrointestinal adenocarcinomas [16]. Our study demonstrates the coexistence of INI-1 and other pathological factors. There was a significant relationship between INI-1 expression and FOXP-1 (r=0.635, p=0.000), EZH-2 (r=0.522, p=0.000), FOXA-1 (r=0.586, p=0.000) and IGF-1R (r=029, p=0.001). The above relationships were confirmed in the logistic regression model, where the increase in INI expression was accompanied by an 8,5 times the expression of FOXA-1 and almost 5 times higher expression of FOXP-1.
Wang et al. concluded that INI1 loss rarely occurs in CRC, which is associated with larger tumor size, higher grade, mismatch repair deficiency, BRAFV600E mutation, and poorer survival [7]. Our studies showed no relationship between increased INI expression and poor survival (p=0,223). Similarly, INI expression did not affect the risk of death (p=0,730). The frequency of INI proteins was not significantly different according to age (p=0.368). Interestingly, there was no higher INI-1 expression in overweight or obese (BMI) patients.
Preclinical data show that IGF-1R is overexpressed in several malignant tumors, including lung, breast, prostate, glioma, and gastrointestinal cancers. Research shows that IGF-1R is overexpressed in many malignant tumors, including - lung, breast, prostate, glioblastoma, and gastrointestinal cancer [17,18]. In our study, the frequency of IGF-1R proteins is not statistically significantly differentiated by age (p=0.276) [19-21]. Our studies showed no relationship between increased IGF-1R expression and poorer survival (p=0,295). Similarly, IGF-1R expression did not affect the risk of death (p=0,147). However, the coexistence of IGF-1R with other pathological factors has also been demonstrated. A relationship was observed between IGF-1R expression and FOXP-1 (r=0,314, p=0,001), EZH-2 (r=0,458, p=0,000), FOXA-1 (r=0,404, p=0,000), and INI-1 (r=0,329, p=0,001). The above relationships were confirmed in the logistic regression model, where the increase in IGF-1R expression was accompanied by over 8 times higher expression of EZH-2 and almost 5 times higher expression of FOXA-1. Interestingly, there was no higher IGF-1R expression in overweight and obese (BMI) patients (p>0,05).
A biomarker must have important characteristics, such as: high sensitivity, specificity, safety, and ease of measurement, and must be useful for diagnosis and therapy. Currently, only MSI and KRAS mutation tests are used for diagnostic and therapeutic purposes in tumors [22].
Currently, personalized medicine is becoming an indispensable tool. Therefore, in-depth tumor analysis should be performed to determine the most appropriate treatment for each patient. Therefore, biomarker determination has a promising future in the diagnosis of CRC, as well as in the development of personalized and targeted therapies.
1. ConclusFOX-family proteins are more common in older people (55 years of age).
2. FOX-family proteins do not impact on general survival in colorectal cancer.
3. None of the tested proteins can be an independent biomarker of colorectal cancer.
Declarations
Funding statement: Project financed under the Jan Kochanowski University grant No SUPB.RN.22.067
Conflict of interest: The authors declare no conflict of interest.
Ethical compliance: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Data access statement: Research data supporting this publication are available from the Monika Kozłowska-Geller repository at located at monika.kozlowska.chir@onet.pl.
References
- Marmol I, Sanchez-de-Diego C, Pradilla Dieste A, Cerrada E, Rodriguez Yoldi MJ. Colorectal carcinoma: A general overview and future perspectives in colorectal cancer. Int J Mol Sci. 2017; 18(1): E197.
- Kozłowska-Geller Monika A, Lewitowicz Piotr, Głuszek Stanisław Z. A five-year follow up study of stage I-IV of rectal cancer with en emphasis on epidermal growth factor over-expression. Pol J Pathol. 2021; 72(1): 1-6. DOI: https: //doi.org/10.5114/pjp.2021.105639
- Kozłowska-Geller Monika, Głuszek Stanisław, Lewitowicz Piotr. Five-year follow up study of stage I-IV rectal cancer including EGFR immunoexpression and p21 immunoactivity. Gastroenterology Rev. 2021; 16 (4): 330-338. DOI: https: //doi.org/10.5114/pg.2021.104980.
- Chen X, Liu J, Zhang Q, Liu B, Cheng Y, et al. Exosome-mediated transfer of miR-93-5p from cancer-associated fibroblasts confer radioresistance in colorectal cancer cells by downregulating FOXA 1 and upregulating TGFB3. J EXP Clin Cancer Res. 2020; 39(1): 65. Doi: 10.1186/s13046-019-1507-2.
- Yanwei Luo, Fengxia Liu, Jinqi Ma, Yunfeng Fu, Rong Gui. A novel epigenetic regulation of circFoxp1 on Foxp1 in colon cancer cells. Cells Death Dis. 2020; 11(9): 782. Doi: 10.1038/s41419-020-03007-6.
- Bohm J, Muenzner J K, Caliskan A, et al. Loss of enhancer of zeste homologue 2 (EZH2) at tumor invasion front is correlated with higher aggressiveness in colorectal cancer cells. J Cancer Res Clin Oncol. 2019; 145(9): 2227-2240. Doi: 10.1007/s00432-019-02977-1.
- Wang J, Andrici J, Sioson L, Clarkson A, Sheen A, Farzin M, et al. Loss of INI1 expression in colorectal carcinoma is associated with high tumor grade, poor survival, BRAFV600E mutation, and mismatch repair deficiency. Hum Pathol. 2016; 55: 83-90. doi: 10.1016/j.humpath.2016.04.018.
- Yingying Sun, Xilin Sun, Baozhong Shen. Molecular Imaging of IGF-1R in Cancer. 2017; 16: 1536012117736648. doi: 10.1177/1536012117736648
- Arnold M, Sierra MS, Laversanne M, Soerjomataram I, Jemal A, et al. Global patterns and trends in colorectal cancer incidence and mortality. Gut. 2017; 66(4): 683–91.
- Zhao J, Lin H, Huang K, Li S. Cancer-associated fibroblast-derived extracellular vesicles carrying IncRNA SNHG3 facilitate colorectal cancer cel proliferation via the miR-34b-5p/HuR/HOXC6 axis. Cell Death Discov. 2022; 8(1): 346.doi: 10.1038/s41420-022-01116-z.
- Koon Henry B, Ippolito Gregory C, Banham Alison H, Tucker Philip W. FOXP1: A potential therapeutic target in cancer. Expert Opin Ther Targets. 2007; 11(7): 955-65. Doi: 10.1517/14728222.11.7.955.
- Hasenpusch C, Fashauer H, Minow A, et al. Digital Health Information Provided by Public Health Stakeholders on Colorectal Cancer Screening: A systematic Evaluaation. Int J Environ Res Public Health. 2022; 19(23): 15624.doi: 10.3390/ijerph192315624.
- Carrasco-Pena F, Bayo-Lozano E, Rodriguez-Barranco M, et al. Adherence to Clinical Practice Guidelines and Colorectal Cancer Survival: A Retrospective High-Resolution Population-Based Study in Spain. Int J Environ Res Public Health. 2020; 17(18): 6697.doi: 10.3390/ijerph17186697.
- Abdel Raouf SM, Ibrahim TR, Abdelaziz La, et al. Prognostic Valuee of TWIST1 and EZH2 Expression in Colon Cancer. J Gastrointest Cancer. 2021; 52(1): 90-98. Doi: 10.1007/s12029-019-00344-44.
- Shao X, Zhao T, Xi L, Zhang Y, He J, et al. LINC00565 promotes the progression of colorectal cancer by upregulating EZH2. Oncol Lett. 2021; 21(1)53. Doi: 10.3892/ol.2020.12314.
- Kohashi K, Oda Y. Oncogenic roles of SMARCB1/INI1 and its deficient tumors. Cancer Sci. 2017; 108(4): 547-552. doi: 10.1111/cas.13173.
- Forbes BE, Blyth AJ, Wit JM. Disorders of IGFs and IGF-1R signaling pathways. Mol Cell Endocrinol. 2020; 518: 111035. Doi: 10.1016/j.mce.2020.111035.
- Zhang Y, Gao C, Cao F, et al. Pan-Cancer Analysis of IGF-1 and IGF-1R as Potential Prognostic Biomarkers and Immunotherapy Targets. Front Oncol. 2021; 11: 755341. Doi: 10.3389/fonc.2021.755341.
- Tufail M, Wu C. Targeting the IGF-1R in prostate and colorectal cancer: Reasons behind trial failure and future directions.Ther Deliv. 2022; 13(3): 167-186. Doi: 10.4155/tde-2021-0060.
- Sun Y, Sun X, Shen B. Molecular Imaging of IGF-1R in Cancer. Mol Imaging. 2017; 16: 1536012117736648. Doi: 10.1177/1536012117736648.
- Zong R, Chen X, Feng J, Xu S. IGF-1R depletion sensitizes colon cancer cell lines radiotherapy. Cancer Biomark. 2021; 32(2): 199-206.doi: 10.3233/CBM-210016.
- Park H, Kim K. Convalescent Hospital Use among Young and Older Female Cancer Survivors. Int J Environ Res Public Health. 2021; 18(5): 2744. Doi: 10.3390/ijerph 18052744.
