
Open Access, Volume 10
Use of a peripheral thrombectomy device in cocaine-induced thrombosis in an anomalous coronary artery
Abharika Sapru; Katherine Lutz; Karla M Asturias; Alexander Heckman; Jeffrey A Marbach*
Division of Cardiology, Knight Cardiovascular Institute, Oregon Health & Science University, Portland, OR 97201, USA.
Jeffrey A Marbach
Division of Cardiology, Knight Cardiovascular Institute, Oregon Health & Science University, 3181 SW Sam Jackson Park Rd, Portland OR 97239, USA.
Email: Marbach@ohsu.edu
Received : August 20, 2024,
Accepted : September 12, 2024
Published : September 16, 2024,
Archived : www.jclinmedcasereports.com
Abstract
We report a case of a 34-year-old male with history notable for cocaine use who presented with STEMI and was found to have significant left main thrombus in the setting of anomalous coronary arteries. Following unsuccessful mechanical aspiration thrombectomy, a larger peripheral mechanical aspiration catheter was used, achieving an improved result. This clinical scenario underscores the difficulties interventionalists face in the setting of large thrombus burden.
Keywords: Thrombus; STEMI; Aspiration thrombectomy; Revascularization.
Abbreviations: STEMI: ST Elevation Myocardial Infarction; LAD: Left Anterior Descending; RCA: Right Coronary Artery; PCI: Percutaneous Coronary Intervention.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Marbach JA (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Sapru A, Lutz K, Asturias KM, Heckman A, Marbach JA. Use of a peripheral thrombectomy device in cocaine-induced thrombosis in an anomalous coronary artery. Open J Clin Med Case Rep. 2024; 2284.
Introduction
Management of large thrombus burden in the setting of acute coronary syndrome has remained a significant challenge for interventionalists. 2021 ACC/AHA/SCAI Guidelines for Coronary Artery Revascularization recommend against routine aspiration thrombectomy prior to PCI in the setting of STEMI due to increased risk of stroke [1] . However, select cases with high thrombus burden may require thrombectomy or alternative methods of thrombus management in order to restore antegrade flow. This case highlights adjunctive use of a peripheral mechanical aspiration catheter for heavy thrombus burden and reviews additional methods for management of the thrombus containing lesion.
Case Report
A 34-year-old male with history of intermittent cocaine use presented to another hospital for 8 hours of chest pain following cocaine use. High sensitivity troponin was 8700, and urine toxicology was positive for amphetamine and cocaine. He was hemodynamically stable with ECG showing ST elevation in anterolateral leads and transferred to the catheterization lab. Echo en route showed Left Ventricular Ejection Fraction (LVEF) of 20% with moderate to severe mitral regurgitation and left ventricular thrombus. Coronary angiogram of the right coronary artery (RCA) revealed an anomalous dual supply left anterior descending artery with takeoff from the RCA (Figure 1A). Left coronary angiography showed significant thrombus in the left main coronary artery and anomalous left circumflex artery (Figure 1B). Mechanical aspiration thrombectomy was pursued with Penumbra CAT Rx thrombectomy catheter. Multiple passes resulted in return of red and white thrombus but unsuccessful antegrade flow. Intravascular ultrasound confirmed small caliber vessel distally, and significant remaining thrombus in the left circumflex and left main (Figure 1C). After minimal improvement with thrombectomy, a balloon pump was placed, and eptifibatide was started. 24 hours later, the patient became hypotensive after balloon pump removal, with elevated lactate to 5.7, followed by escalation of vasopressors and subsequent intubation. A multidisciplinary shock call was made to our hospital. Balloon pump was replaced, and the patient was transferred for escalation of therapy.
Repeat coronary angiogram on presentation showed significant thrombus burden of the left main into the left circumflex artery (Figures 2A and 2B). Penumbra CAT Rx thrombectomy catheter was used, which kept clogging with thrombus. Femoral access was upsized to an 8F system, and a larger peripheral penumbra CAT 6 aspiration catheter was used due to the internal diameter (5.4F vs 3.35F) which would provide both more suction power and larger area to prevent clogging. This upsizing resulted in successful aspiration of multiple large thrombi with improved antegrade flow. The left main lesion (Figure 2C) was predilated and 3.0x 18 Onyx Frontier stent was deployed and post-dilated with 4.0 x 8 mm NC balloon (Figure 2D). No reflow was treated with nitroprusside, adenosine, and epinephrine. After returning to the ICU, the balloon pump was exchanged for Impella 5.5, and LVAD was placed in the subsequent weeks. The patient had a prolonged hospitalization and was on dialysis until close to discharge approximately 2 months after admission. The patient is now working toward heart transplant.
Table 1: Thrombus revascularization strategies.
| Strategy | Impact |
|---|---|
| Pharmacologic | |
| Early pharmacotherapy with potent P2Y12inhibitor such as ticagreloror prasugrel | Potent platelet inhibition |
| Systemic or intracoronary glycoprotein IIb/IIIa inhibitors | Potent platelet inhibition |
| Intracoronary lytics | Local delivery of fibrinolytic agentto dissolve thrombus |
| Intracoronary vasodilators | Decreases risk of distal embolization and no-reflow |
| Thrombus removal/ retrieval strategies | |
| Manual aspiration thrombectomy | Removal of thrombus manually with negative pressure applied by syringe |
| Mechanical aspiration thrombectomy | Continuous suction applied through a mechanically-operated device |
| Upsize to larger, peripheral aspiration catheter | Avoidance of clogging aspiration catheter and increased suction power |
| Self-expanding stentretriever combined withmechanical aspiration | Thrombus is captured with the stentretriever combined with mechanical aspiration to prevent thrombus embolization |
| Thrombus aspiration catheter-assisted twisting wire | Useof second shaped guidewire to twist around the first wire that is alreadypassing through the thrombus in a helicalfashion to retrieve the thrombus intothe guide extension for removal |
| Mechanical physical dissolution devices | |
| Rheolytic therapy (Angiojet) | Mechanically disrupts clot with injection of high pressure saline, creating Venturi effect, followed by aspirationof thrombus through the proximal port |
| Helical cutting withinprotective housing (x-sizer thrombectomy catheter) | Helical cuttingresults in fragmentation of clot followed by removal |
| Laser (Excimer laser) | Separate and dissolve thrombus |
| Stroke/distal embolization avoidance strategies | |
| Embolic protection device | Decreases distal embolization |
| Covered/mesh covered stent | Retain thrombus against vessel wall |
| Use of guideextension and/or deep-seated guide catheter | Avoid risk of stroke |
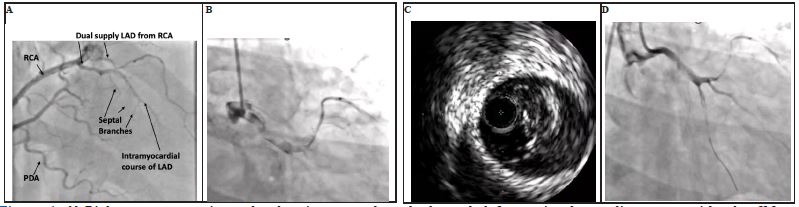
Figure 1: A) Right coronary angiography showing anomalous dual supply left anterior descending artery with takeoff from the right coronary artery. B) Initial injection of the left coronary system showing large thrombus burden throughout. C) Intravascular ultrasound (IVUS) with significant thrombus burden in left main. D) Final injection of the left coronary system following multiple passes with CAT Rx aspiration catheter.
RCA: Right Coronary Artery; LAD: Left Anterior Descending Artery; PDA: Posterior Descending Artery
RCA: Right Coronary Artery; LAD: Left Anterior Descending Artery; PDA: Posterior Descending Artery
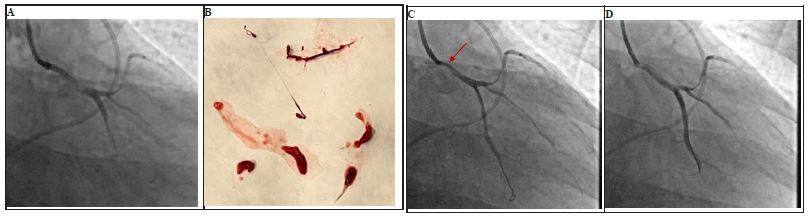
Figure 2: A) First injection of left coronary system showing large thrombus burden. B) Removal of significant red and white thrombi following upsizing aspiration thrombectomy catheter to the peripheral aspiration catheter, Penumbra CAT 6. C) Significant left main lesion following aspiration thrombectomy (red arrow). D) Final image after pre-dilating and stenting of left main lesion with 3.0 mm x 18 mm Onyx Frontier stent and post-dilating to 4.0 mm.
Discussion
This case demonstrates the challenges of dealing with significant thrombus burden and shows an improved result with upsizing to a peripheral thrombectomy catheter in the setting of significant thrombus burden as an alternative strategy. A Class 3 recommendation against the use of routine aspiration thrombectomy resulted from the TASTE and TOTAL trials which utilized manual aspiration thrombectomy only in every patient, which may not be warranted nor the optimal approach for each patient. There are pharmacologic therapies, mechanical thrombectomy, mechanical physical dissolution devices, and other novel techniques which could be combined with a stroke avoidant strategy that may facilitate a more successful and safe result for patients (Table 1). A targeted thrombus revascularization strategy may be applied for select patients to reduce thrombus burden as a barrier to antegrade flow, reduce the threat of thrombotic embolization, treat stent thrombosis, or remove thrombotic emboli lodged in a coronary artery or saphenous vein graft.
Pharmacotherapy may be considered initially, which includes early administration of dual antiplatelet therapy, consideration of potent P2Y12 inhibitor such as ticagrelor or prasugrel, use of either systemic or intracoronary glycoprotein IIb/IIIa inhibitors, intracoronary lytics, and intracoronary vasodilators to decrease risk of distal embolization and no-reflow [2] . Upstream use of glycoprotein IIb/IIIa inhibitors is not recommended and should be considered as a bailout strategy only and for higher grades of thrombus. Depending on presence of ongoing ischemia, a deferred stenting strategy where antiplatelet therapy and prolonged GPIIb/IIIa inhibitor therapy for 24-48 hours could be considered, although is not recommended in the current guidelines. Intracoronary thrombolysis has previously shown mixed results; however, a meta-analysis of 1873 STEMI patients from 13 randomized controlled trials showed a significant reduction in major adverse cardiovascular events compared to placebo with no difference in rates of major bleeding [3].
Thrombus aspiration/retrieval can be considered next, and in our case, upsizing to a larger peripheral catheter provided both more powerful aspiration as well as a larger lumen size to avoid clogging of the catheter. There have been several case reports utilizing innovative techniques for thrombus retrieval including use of a self-expanding stent retriever to capture thrombus for retrieval into the guide [4]. Additionally, a thrombus aspiration catheter-assisted twisting wire technique can be considered which utilizes a second twisted wire around the first wire passed through the thrombus to grab and entrap the thrombus for retrieval into a guide extension followed by removal [5] .
If aspiration thrombectomy is unsuccessful, there are mechanical physical dissolution devices including those which utilize rheolytic therapy, helical cutting within protective housing, and laser to separate and dissolve thrombus. Revascularization strategies that utilize more than pharmacotherapy should factor in ways to mitigate stroke risk including use of a guide extension, deep-seated guide catheter, or embolic protection device. A covered or mesh covered stent can also be used to retain the thrombus against the vessel wall.
Conclusion
In select patients, it is critical to consider adjunctive therapies for large thrombus burden, including pharmacotherapy, thrombus removal/retrieval strategies, mechanical dissolution, and embolic protection. Further research investigating optimal management is warranted.
Declarations
Credit authorship contribution statement: Abharika Sapru: Writing- original draft. Katherine Lutz: Writing- review & editing. Karla M. Asturias MD: Writing-review & editing. Alexander Heckman: Writing-review & editing. Jeffrey A. Marbach: Writing-review & editing, Supervision.
Declaration of competing interest: We have no conflicts of interest to disclose. We have no financial or other interest in the product or distributor of the product.
References
- Lawton JS, Tamis-Holland JE, Bangalore S, et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022: E18-114. Doi: 10.1161/CIR.0000000000001038.
- Kumar V, Sharma AK, Kumar T, Nath RK. Large intracoronary thrombus and its management during primary PCI. Indian Heart J. 2020; 72(6): 508. Doi: 10.1016/J.IHJ.2020.11.009.
- Alexiou S, Patoulias D, Theodoropoulos K, Kassimis G. Intracoronary thrombolysis facilitated primary percutaneous coronary intervention in ST-segment elevation myocardial infarction patients: An updated meta-analysis of randomized controlled trials. Eur Heart J 2022; 43(Supplement_2). Doi: 10.1093/EURHEARTJ/EHAC544.1389.
- Crimi G, Moramarco L, Mandurino-Mirizzi A, Quaretti P, Ferrario M. The combined use of stent retriever and neuro-aspiration as successful bail-out reperfusion strategy in a patient with embolic myocardial infarction. Catheterization and Cardiovascular Interventions. 2019; 94(2): E78-81. Doi: 10.1002/CCD.28167.
- Zou YL, Li JQ, Gong YT, Sun DH, Li Y. A novel treatment of refractory coronary embolism: thrombus aspiration catheter-assisted twisting wire technique. J Geriatr Cardiol. 2020; 17(2): 110. Doi: 10.11909/J.ISSN.1671-5411.2020.02.005.
