
Open Access, Volume 10
Spontaneous haemoperitoneum in the second trimester of pregnancy
Jonathan Gaughran1,2*; Alexandra Cocking1; Sian Mitchell1,2; Ahmad Sayasneh2,3
1Guy’s & St Thomas’ Hospitals, Women’s Health, London, UK.
2King’s College London, School of Life Sciences, London, UK.
3Gynaecological Oncology Department, Guy’s and St Thomas’ Hospitals, London, UK.
Jonathan Gaughran
Guy’s & St Thomas’ Hospitals, Women’s Health, London, UK.
Email: gaughraj@tcd.ie
Received : August 14, 2024,
Accepted : September 06, 2024
Published : September 16, 2024,
Archived : www.jclinmedcasereports.com
Abstract
We report the case of a 34-year-old woman who presented to secondary care at 18 weeks’ gestation with acute abdominal pain. A diagnosis of haemoperitoneum secondary to a ruptured ovarian cyst was made and conservative management undertaken. Two weeks following discharge, the patient re-presented with Pre-term Pre-Labour Rupture of Membranes (PPROM) and went on to have an emergency Caesarean Section at 26+3 weeks’ gestation for presumed chorioamnionitis. Both mother and baby made a good recovery. We explore haemoperitoneum in pregnancy and look at the challenges faced in its diagnosis and management. We also consider the consequences it may have for the ongoing pregnancy.
Keywords: Adnexa; Haemoperitoneum; Pregnancy; Prematurity; Chorioamnionitis; Cyst; Ovary.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Gaughran J (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Gaughran J, Cocking A, Mitchell S, Sayasneh A. Spontaneous haemoperitoneum in the second trimester of pregnancy. Open J Clin Med Case Rep. 2024; 2282.
Background
Spontaneous haemoperitoneum during pregnancy is rare, with an estimated incidence of 0.04/1000 births, and poses both a diagnostic and therapeutic challenge [1]. It is defined as the presence of blood within the peritoneal cavity from a non-traumatic cause and may be fatal to both mother and fetus [2]. Common causes include spontaneous rupture of: blood vessels, aneurysms, cysts and tumours; coagulopathies and endometriosis. Pregnancy specific causes include rupture of pregnancy related adnexal masses, ectopic pregnancies, uterine dehiscence and abnormally invasive placentas [2,3]. Although the mechanism is not understood, Artificial Reproductive Techniques (ART) are thought to be an additional risk factor [2,4]. Believed to be due to improvements in both imaging and operative practices, maternal mortality rates have decreased from 49.3% to 3.6% over the last 70 years [5,6]. Neonatal mortality however, remains high at an estimated 31-36% [3].
Symptoms are often non-specific and include abdominal pain, gastrointestinal upset, and in severe cases, symptoms associated with haemorrhagic shock [7,3]. Physical signs associated with haemoperitoneum are bruising around the umbilicus (Cullen’s sign) and over the flanks (Grey Turner’s Sign), as well as alterations in maternal observations such as tachycardia and hypotension [8]. Alterations in the fetal heart rate may be observed and investigations may reveal an acute drop in maternal haemoglobin [7]. Ultrasound is usually the first imaging modality applied due to accessibility and safety in pregnancy. It can detect free fluid within the abdominal cavity with a sensitivity and specificity of >90% [9,10]. However, cross-sectional imaging in the form of CT or MRI may be required to confirm this fluid to be haemorrhagic and to localise the source of bleeding [11].
Laparoscopy or laparotomy may be necessary to ascertain the precise bleeding point and offer the advantage of allowing treatment and cessation of bleeding [7]. However, in patients who lack signs of maternal or fetal compromise, conservative management with analgesia and close observation is often favoured due to increased morbidity and mortality associated with operative intervention during pregnancy [7,10].
Case Presentation
A woman in her mid 30’s presented to the Maternity Assessment Unit (MAU) of a large teaching hospital at 18 weeks’ gestation with acute abdominal pain. The pain had begun one day prior, was localised to the suprapubic area and was associated with nausea, but no vomiting. There were no other symptoms. On examination there was objective mild suprapubic tenderness, observations were within normal limits, and urine dip test was negative. The fetal heart rate was within normal range for gestation. No blood tests were performed. The pregnancy had been uncomplicated prior to this presentation. One previous pregnancy resulted in an early miscarriage managed by an uncomplicated surgical evacuation. The only comorbidities were polycystic ovarian syndrome and anxiety. An impression of pelvic girdle pain was reached and the patient discharged with simple analgesia.
The patient re-presented three days later with generalised, severe abdominal pain. On examination, there was maximum tenderness in the right upper quadrant and Cullen’s sign was positive. Maternal observations were within normal range and fetal heart rate was normal. Urgent bloods (Full Blood Count [FBC] Urea & Electrolytes [U&Es], Liver Function Tests [LFTs], Amylase, C-Reactive Protein [CRP], lactate & Group & Save) were sent (Table 1).
A trans-abdominal ultrasound scan performed by a level II ultrasound practitioner which was reported as ‘There is ascites with echogenic material, likely proteinaceous in nature. There is no evidence of gallstones or cholecystitis. The aorta, spleen, kidneys and pancreas appeared normal; however the appendix could not be visualised (Figure 1).
Table 1: Blood results at antenatal booking and throughout first admission.
| Investigation | Booking | Admission | Day 2 | Day 3 | Day 4 | Day 5 |
|---|---|---|---|---|---|---|
| Haemoglobin | 119 | 94 | 78 | 96 | 101 | 104 |
| Mean CellVolume | 89 | 89 | 89 | 89 | 89 | 88 |
| White CellCount | 6.7 | 14.6 | 8.6 | 8 | 8.5 | 8.6 |
| Neutrophils | 4.4 | 13.3 | 6.6 | 5.3 | 6.4 | 6.5 |
| Platelets | 300 | 306 | 249 | 228 | 274 | 346 |
| Sodium | 135 | 136 | 136 | |||
| Potassium | 4.4 | 3.9 | 4.0 | |||
| Creatinine | 38 | 41 | 39 | |||
| C-Reactive Protein | 8 | 23 | 27 | |||
| Bilirubin | 3 | 4 | 10 | |||
| Alanine Transaminase | 12 | 13 | 15 | |||
| Alkaline Phosphatase | 50 | 46 | 64 | |||
| Amylase | 35 | |||||
| Lactate | 2.8 |

Figure 1: Transabdominal ultrasound showing intra-abdominal mixed echogenic fluid.
Due to ongoing pain and no clear diagnosis, bloods were repeated the following day (Table 1). An MRI abdomen, pelvis, uterus and fetus without contrast was performed which was reported as ‘There is ascites which is of intermediate to high T1 signal, possibly representing proteinaceous content. Haemorrhagic fluid is felt less likely. All other intra-abdominal organs have normal appearances and both ovaries appear normal. No cause of the patient’s abdominal pain is identified. There is an unusual horizontal band like structure in the inferior right posterior aspect of the uterine cavity that appears to be separating the cavity in two. The fetus is located in the superior cavity and surrounded by a limited amount of amniotic fluid; the inferior cavity is filled with amniotic fluid. It is unclear if the two spaces communicate. This may represent either an amniotic band or a uterine adhesion’.
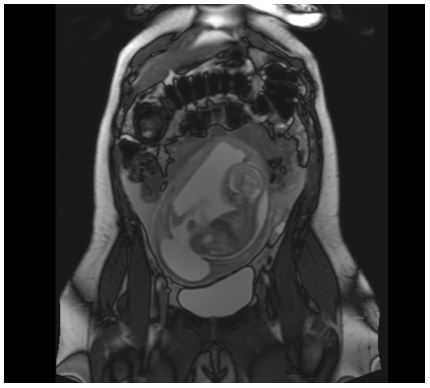
Figure 2: MRI showing intrauterine pregnancy and high T1 signal intra-abdominal fluid.
Finally, a bedside trans-abdominal ultrasound scan by a level III gynaecological ultrasound practitioner was requested. This was reported as:'There is a significant volume of mixed echogenic free fluid in the abdominal cavity in keeping with blood. The right ovary contains a 10 mm well demarcated cystic structure containing mixed echogenic material with a breach of the ovarian serosa suggestive of cyst rupture’.
Based on the results of the imaging, and the acute drop in haemoglobin an impression of haemoperitoneum, secondary to ovarian cyst rupture was reached. The patient received 2 units of cross-matched red blood cells and regular paracetamol and opioids. As the Hb did not decrease post transfusion and the pain began to settle, a decision was made to manage the haemoperitoneum conservatively, and the patient was discharged well on day 5.
Two weeks following discharge, at 22+2 weeks gestation, the patient re-presented to the MAU reporting clear fluid loss per vagina and ongoing lower abdominal pain. Speculum examination revealed the cervix was dilated to 1 cm, membranes could be seen bulging, and clear flood was pooling in the vagina. Maternal observations were all in normal range, bloods were unremarkable (Table 2) and the fetal heart rate was reported as normal.
A diagnosis of PPROM was made. The patient was commenced on erythromycin 250 mg QDS for 7 days as per the ORACLE trial results and admitted for observations [14]. During this time both the prognosis and possibility of termination of pregnancy was discussed, but a decision was made to continue the pregnancy. Following 3 days of observation the patient was discharged with a plan for twice weekly bloods and clinical review on the MAU. At 24 week’s gestation a course of intramuscular corticosteroids were administered for fetal lung maturity.
At 26+3 week’s gestation the patient’s inflammatory markers rose (Table 2), but maternal observations and clinical examination remained unremarkable. A fetal ultrasound scan demonstrated a viable fetus in transverse lie, anhydramnios with normal growth and Dopplers. Due to a further rise in inflammatory markers on Day 1 following readmission, an impression of evolving chorioamnionitis was made and a category three Caesarean-Section was offered and accepted.
Table 2: Blood results during second admission.
| Investigation | Readmission | Day1 | Day2 | Day3 |
|---|---|---|---|---|
| Hb | 108 | 107 | 97 | 91 |
| MCV | 90 | 91 | 88 | 89 |
| WCC | 10.5 | 12.8 | 18 | 9.6 |
| Neutrophils | 7.4 | 9.5 | 14.9 | 6.2 |
| Plt | 427 | 305 | 254 | 225 |
| CRP | 8 | 63 | 154 | 125 |
At Caesarean Section, upon opening the peritoneal cavity, a large amount of both fresh and old blood was evacuated. The total measured blood loss at the end of surgery was 2.3 litres. A live fetus was delivered via a classical incision with APGARs of 2 at 1 minute, 8 at 5 minutes and 9 at 10 minutes. An arterial blood gas was obtained demonstrating a pH of 7.313 (venous was unobtainable) and birth weight was recorded as 1030 g. The baby was admitted to the Neonatal Intensive Care Unit (NICU) intubated and ventilated. Both ovaries were reported as grossly normal and there was no evidence of ongoing bleeding from any site within the abdomen. The peritoneal cavity was washed out with warm water, closed, and the patient transfused 2 units of cross matched blood intraoperatively.
The patient was discharged well on day 4 post-surgery. The baby remained in NICU for 3 months being treated for respiratory distress syndrome, sepsis and establishing feeding, but was discharged, breathing and feeding independently with no detectable neurological sequelae.
Discussion
This case is of interest for a number of reasons. It reminds us that although haemoperitoneum in pregnancy is rare, it is an important differential diagnosis in patients with abdominal pain and/or haemodynamic instability, due to the associated maternal and fetal morbidity. It also highlights the diagnostic challenges of this scenario, and raises questions over the impact it may have on the remainder of the pregnancy.
Lier et al. performed a systematic review of 59 cases of spontaneous haemoperitoneum in pregnancy [7]. The majority presented with acute abdominal pain, hypovolaemic shock, fetal distress and acute anaemia. In 76.3% of these cases, operative management was undertaken. Of those that underwent surgery, the origin of bleeding was ruptured utero-ovarian vessels in 56.8%, endometriotic implants in 21.6%, haemorrhagic nodules of decidualised cells in 2%, or a combination in 19.6%. One maternal death was reported, however perinatal mortality was 26.9%. They concluded that spontaneous haemoperitoneum is a serious complication of pregnancy with a high rate of adverse outcomes and that early recognition is key. Spontaneous haemoperitoneum and its source can be difficult to identify in pregnant women and this can lead to a dangerous delay in diagnosis. Lier et al. reported that in cases of proven haemoperitoneum at surgery, imaging confirmed free peritoneal fluid in only 62.7% of cases; 89.2% of which had ultrasound alone [7]. Sonography is often the first line investigation for abdominal pain in pregnancy due to the minimal adverse effects on the fetus and its availability. The sensitivity and specificity of ultrasound in detection of haemoperitoneum is >90% in the non-pregnant population [9]. However, pregnancy adds diagnostic challenges due to displacement of structures by the expanding uterus and as this case demonstrated, it can be operator dependant and may not detect the source of bleeding [2,15]. As such, cross-sectional imaging may be required. MRI is used preferentially as it can image deep soft tissue structures without ionising radiation and does not have any pregnancy-specific contraindications [16]. Limitations of MRI however, include high cost, long scan time, fetal movement artefact, and the fact it is often not readily available out of hours [15,17]. In cases where patients are unstable and a quick diagnosis is needed, CT with or without contrast can be considered to find an active bleeding point, but only after careful discussion with the patient regarding the potential increased risk of childhood cancer associated with radiation exposure in utero [15]. In this case, MRI was used as the initial cross-sectional imaging modality so as to avoid ionising radiation but it was not able to identify the free fluid as blood, nor the source of bleeding. Unfortunately, there is little guidance in the literature as to whether CT or MRI is superior when trying to identify the source of active intra-abdominal bleeding in a pregnant patient. Clinicians must carefully balance the risks of certain imaging modalities against the benefits of a timely diagnosis as in the case of spontaneous haemoperitoneum, a delayed diagnosis can be catastrophic. The recent MBRRACE report of 2021 highlighted this and have advised that clear guidance is developed on imaging in pregnancy [18].
There is conflicting opinion in the literature about what constitutes optimal management. Xu et al. [3] recommend exploratory laparotomy at the time of diagnosis of haemoperitoneum in all patients, however both Brossens et al. and Lier et al. suggest a role for conservative management in cases where mother and fetus show no signs of haemodynamic compromise [19,7]. In this case, conservative management was favoured over operative intervention after discussion with a multidisciplinary team. In Lier et al. systematic review of 59 cases of spontaneous haemoperitoneum in pregnancy, they reported that 45 (76%) of patients underwent laparoscopy or laparotomy due to signs of maternal haemodynamic instability or fetal distress. In the cases that were managed surgically, only 15.6% had a live birth, and only 11% reached 37 weeks’ gestation. Whether this was a result of operative intervention, or due to the severity of materno-fetal compromise at the outset of surgery is unclear. It is however known that operative intervention in pregnancy carries additional risks than in the non-pregnant population [10]. As such, it is suggested in the literature, and as was adopted in this case, where there is no evidence of hypovolaemic shock or fetal distress, conservative management is a reasonable approach. Clinicians should however counsel patients about the potential that recovery can be complicated by an infected haematoma or recurrence of haemoperitoneum later in pregnancy [7]. In this case, avoiding operative intervention allowed the patient to be spared potential surgical morbidity and the pregnancy continued to post viable gestational age. It is impossible to state if the outcome would have been different should surgery have been undertaken.
It is unclear whether the PPROM and premature delivery were associated with haemoperitoneum in this case. PPROM is believed to complicate between 1-4% of pregnancies globally [20]. Risk factors include cervical insufficiency, cigarette smoking during pregnancy, low maternal BMI, polyhydramnios, multiple gestations and advanced maternal age [21]. In the absence of any of these risk factors, we believe the uterine abnormality and/or haemoperitoneum contributed. The horizonal uterine bands were believed to be either a uterine adhesion or an amniotic band. The presence of an intra-uterine adhesion may be explained by the history of surgical management of miscarriage which is known to be a risk factor for this [22]. A recent literature review of post-traumatic intrauterine adhesions (Asherman syndrome) by Yu et al. found a 23% increased risk of preterm birth [23]. Amniotic bands are thought to result from damage to the amnion early in pregnancy, resulting in loose fibrous bands [24]. These bands can wrap around the foetus, leading to congenital abnormalities and have been shown to increase the risk of preterm delivery [25].
Neither a band nor an adhesion were seen at Caesarean Section, however both may have been divided by the surgeon’s hand delivering the fetus. In relation to haemoperitoneum, a recent case series by Lier et al. suggested a 54.5% incidence of pre-term births in those with haemoperitoneum in pregnancy [26]. The mechanism of this is believed to be uterine hypertonus caused by the presence of blood within the peritoneum, which leads to contractions and subsequent cervical dilatation [27].
In this case, haemoperitoneum was believed to be secondary to a ruptured ovarian cyst. The incidence of adnexal masses in pregnancy is between 0.19 to 8.8% [28]. The most common pregnancy-associated ovarian masses are functional cysts such as corpora lutea which are hormonally influenced. While the majority regress by 16 weeks’ gestation, they can rupture and haemorrhage [29]. Another common type of adnexal mass found in pregnancy are endometriomas. These non-physiological masses may undergo rapid growth and structural transformation secondary to raised progesterone concentrations which can lead to rupture and haemoperitoneum [29-31]. In a recent systematic review of haemoperitoneum in pregnancy, 55.9% of cases were related to endometriosis [7]. In the case described above, there was no history of endometriosis and no signs of it detected at Caesarean Section, as such the presumption that this was due to a ruptured physiological cyst that had resolved by time of laparotomy. In the absence of significant bleeding secondary to rupture, or concern about torsion or malignancy, adnexal masses diagnosed in pregnancy should be managed conservatively [10].
We conclude that although rare, all clinicians should include spontaneous haemoperitoneum as a differential diagnosis when assessing acute abdominal pain in pregnancy. Due to the high incidence of adverse outcomes, it is imperative that it is diagnosed quickly and managed effectively. More research is needed regarding optimal imaging modalities and management which could serve the basis for clinical guidelines. At present it is unknown if conservative management of haemoperitoneum confers an ongoing risk for PPROM.
References
- Mazzocco MI, Donati S, Maraschini A, Corsi E, Colciago E, et al. Spontaneous hemoperitoneum in pregnancy: Italian prospective population‐based cohort study. Acta Obstetricia et Gynecologica Scandinavica. 2022; 101(11): 1220-6.
- Lucey BC, Varghese JC, Anderson SW, Soto JA. Spontaneous hemoperitoneum: A bloody mess. Emergency Radiology. 2007; 14(2): 65-75.
- Xu Y, Zhou Y, Xie J, Yin X, Zhang X. Intraperitoneal haemorrhage during pregnancy and parturition. Medicine. 2019; 98(35): e16300.
- Ivo Brosens, Lier MCI, Mijatovic V, Marwan Habiba, Benagiano G. Severe spontaneous hemoperitoneum in pregnancy may be linked to in vitro fertilization in patients with endometriosis: a systematic review. 2016; 106(3): 692-703.
- C. Paul Hodgkinson, Christensen RC. Haemorrhage from Ruptured Uteroovarian Veins During Pregnancy. American Journal of Obstetrics and Gynaecology. 1950; 59(5): 1112-7.
- Takahashi T, Kikuchi S. Spontaneous rupture of utero-ovarian vein in the 33rd week of pregnancy. Asia Oceania J Obstet Gynaecol. 1985; 11(3): 387-92. doi: 10.1111/j.1447-0756.1985.tb00759.x. PMID: 4084106.
- Lier MCI, Malik RF, Ket JCF, Lambalk CB, Brosens IA, et al. Spontaneous hemoperitoneum in pregnancy (SHiP) and endometriosis- A systematic review of the recent literature. European Journal of Obstetrics & Gynecology and Reproductive Biology. 2017; 219: 57-65.
- Wright WF. Cullen Sign and Grey Turner Sign Revisited. The Journal of the American Osteopathic Association. 2016; 116(6): 398.
- Hannu Paajanen, Lahti P, Isto Nordback. Sensitivity of transabdominal ultrasonography in detection of intraperitoneal fluid in humans. European Radiology. 1999; 9(7): 1423-5.
- Gaughran JE, Naji O, Al Sabbagh MQ, Sayasneh A. Is Ultrasound a Reliable and Reproducible Method for Assessing Adnexal Masses in Pregnancy? A Systematic Review. Cureus. 2021.
- Kanakaris NK, Roberts CS, Giannoudis PV. Pregnancy-related pelvic girdle pain: an update. BMC Med. 2011; 9: 15. doi: 10.1186/1741-7015-9-15. PMID: 21324134; PMCID: PMC3050758.
- Gaughran J, Chung B, Lyne T, Syeda N, Field D, et al. Is routine urine dip stick testing justified in asymptomatic women in early pregnancy? Int J Reprod Contracept Obstet Gynecol. 2021; 10: 17-21.
- Zachariah SK, Fenn M, Jacob K, Arthungal SA, Zachariah SA. Management of acute abdomen in pregnancy: current perspectives. International Journal of Women’s Health. 2019; 11: 119-34.
- Kenyon S, Taylor D, Tarnow-Mordi W. Broad-spectrum antibiotics for preterm, prelabour rupture of fetal membranes: the ORACLE I randomised trial. The Lancet. 2001; 357(9261): 979-88.
- Wiles R, Hankinson B, Benbow E, Sharp A. Making decisions about radiological imaging in pregnancy. BMJ. 2022; 377: e070486.
- Committee Opinion No. 723: Guidelines for Diagnostic Imaging during Pregnancy and Lactation. Obstet Gynecol. 2017; 130(4): e210-e216. doi: 10.1097/AOG.0000000000002355. Erratum in: Obstet Gynecol. 2018; 132(3): 786. PMID: 28937575.
- Adam R, Ahmed M. MRI Limitations: The main aspects and resolving techniques. Indian Journal of Applied Research. 2020; 10(9): 71-73.
- Knight M, Bunch K, Tuffnell D, Patel R, Shakespeare J, et al. on behalf of MBRRACE-UK. Saving Lives, Improving Mothers’ Care - CORE report lessons learned to inform maternity care from the UK and Ireland Confidential Enquiries into Maternal Deaths and Morbidity 2017-19. Oxford: National Perinatal Epidemiology Unit, University of Oxford. 2021.
- Brosens IA, Fusi L, Brosens JJ. Endometriosis is a risk factor for spontaneous hemoperitoneum during pregnancy. Fertility and Sterility. 2009; 92(4): 1243-5..
- Jena BH, Biks GA, Gete YK, Gelaye KA. Incidence of preterm premature rupture of membranes and its association with inter-pregnancy interval: a prospective cohort study. Scientific Reports. 2022; 12(1).
- Enjamo M, Deribew A, Semagn S, Mareg M. Determinants of Premature Rupture of Membrane (PROM) Among Pregnant Women in Southern Ethiopia: A Case-Control Study. International Journal of Women’s Health. 2022; 14: 455-66.
- Deans R, Abbott J. Review of Intrauterine Adhesions. Journal of Minimally Invasive Gynecology. 2010; 17(5): 555-69.
- Asherman syndrome-one century later. Fertility and Sterility. 2008; 89(4): 759-79.
- Singh AP, Gorla SR. Amniotic Band Syndrome [Internet]. PubMed. Treasure Island (FL): StatPearls Publishing. 2022. Available from: https: //www.ncbi.nlm.nih.gov/books/NBK545283/
- Wehbeh H, Fleisher J, Karimi A, Mathony A, Minkoff H. The relationship between the ultrasonographic diagnosis of innocent amniotic band development and pregnancy outcomes. Obstet Gynecol. 1993; 81(4): 565-8. PMID: 8459968.
- Lier M, Malik RF, van Waesberghe J, Maas JW, van Rumpt-van de Geest DA, et al. Spontaneous haemoperitoneum in pregnancy and endometriosis: A case series. BJOG: An international journal of obstetrics and gynaecology. 2017; 124(2): 306-12.
- Miki H, Tanaka H, Yutaka Osuga, Miura K, Saito S, et al. Nationwide survey (Japan) on spontaneous hemoperitoneum in pregnancy. Journal of Obstetrics and Gynaecology Research. 2021; 47(8): 2646-52.
- Res Clin Obstet Gynaecol. 2009; 23(4): 539-48. doi: 10.1016/j.bpobgyn.2009.01.009.
- Senarath S, Ades A, Nanayakkara P. Ovarian cysts in pregnancy: a narrative review. Journal of Obstetrics and Gynaecology. 2020; 41(2): 169-75.
- Brosens I, Brosens JJ, Fusi L, Al-Sabbagh M, Kuroda K, et al. Risks of adverse pregnancy outcome in endometriosis. Fertility and Sterility. 2012; 98(1): 30-5.
- Gaughran J Naji O, Murad A, Sayasneh A. Can ultrasound reliably assess ovarian endometriomas in pregnancy? A systematic review, EGO European Gynecology and Obstetrics. 2022); 2022/01: 002-011
