
Open Access, Volume 10
Treatment of drug-induced erythema multiforme: Case report
Ambika Murari1*; Rajendragouda Patil2; Arjit Vihan1; Angshuman Sarma1; Paridhi Agarwal1
1Department of Oral Medicine and Radiology, Kothiwal Dental College and Research Centre, Moradabad, India.
2Professor and Head, Department of Oral Medicine and Radiology, Kothiwal Dental College and Research Centre, Moradabad, India.
Ambika Murari
Department of Oral Medicine and Radiology, Kothiwal Dental College and Research Centre, Moradabad, India.
Tel: 9719961934;
Email: ambikaj27@gmail.com
Received : August 13, 2024,
Accepted : September 04, 2024
Published : September 16, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Erythema Multiforme (EM) is an acute condition driven by the immune system, featuring the rapid emergence of distinct target-like lesions on the skin and mucous membranes. It usually presents symmetrically, most commonly affecting the extremities, and its severity can range from mild (EM minor) to severe (EM major). The condition is usually triggered by infections, especially the Herpes Simplex Virus (HSV), but can also be caused by certain medications, vaccines, and other factors. Its pathogenesis involves a complex interaction between the immune system and epithelial cells, resulting in cell-mediated cytotoxic responses. Clinically, patients may exhibit initial symptoms such as fever, malaise, and upper respiratory issues, followed by the development of lesions that progress over several days. Diagnosis primarily relies on clinical evaluation, complemented by histopathological evidence showing interface dermatitis with necrotic keratinocytes. Management strategies aim to identify and remove the triggering factor, offering symptomatic relief through antihistamines, analgesics, and topical corticosteroids for mild cases, while severe cases may require systemic corticosteroids or immunosuppressive agents. Here, we are presenting a case of erythema multiforme in 27 years 27-year-old male.
Keywords: Erythema multiforme; Emergency; Skin; Patients.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Murari A (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Murari A, Patil R, Vihan A, Sarma A, Agarwal P. Treatment of drug-induced erythema multiforme: Case report. Open J Clin Med Case Rep. 2024; 2281.
Introduction
The first documented description of this condition dates back to Ferdin in 1860. In medical literature, it is often associated with herpes viruses, with the term «multiforme» reflecting the disease’s characteristic variability. Other triggers include certain medications, autoimmune conditions, radiation, vaccinations, pregnancy, menstruation, and exposure to food or chemical additives. Another common association, particularly in children, is with the bacterium Mycoplasma pneumonia [1].
The clinical manifestations of EM involve the activation of cytotoxic T lymphocytes within the epithelium, which trigger apoptosis in keratinocytes, resulting in necrosis of surrounding cells. Typically, EM begins with symmetrical lesions on the extremities, characterized by “target” patterns that tend to spread inward towards the trunk. Skin lesions associated with EM typically remain stable for at least seven days, a distinguishing feature that helps differentiate it from other immune-mediated disorders like urticaria and allergic rashes. Initial management of EM focuses on symptomatic relief through the use of topical and systemic steroids, while also emphasising the avoidance of known triggers such as medications [2].
Here, describing a case of drug-induced erythema multiforme in a 27-year-old male patient, predominantly affecting the oral cavity.
Case Report
A 27-year-old male reported with a chief complaint of ulcerations since 1 month. The patient gave a history of fever 1 month back for that he took medicine from the local drug store and got relief from the fever. But soon after that, he starts noticing multiple painful ulcers in his oral cavity and lip region. Which later involved the whole of the oral cavity. The patient was unable to take food due to painful ulcerations. Medical history revealed that the patient took paracetamol 500 mg to cure the fever. The patient also gives a history of the same lesion in the mouth 8 years back which was extended to the trunk region. Dental history was not contributory. Personal history revealed that the patient had a habit of chewing tobacco 4-5 packets per day for 7 years. But now in 1 month, he discontinued this habit. On general examination, the patient was moderately built and well-nourished. And well-oriented to the time, place and thing. The patient was afebrile with all vital signs within normal limits.

Figure 1: Extra-oral picture pre-treatment.
On extra-oral examination, a brownish-black crested, irregular lesion was seen over the upper and lower lip region measuring 1 x 0.5 cm (in upper lip) and 0.5 x 0.5 cm (in lower lip) at the middle 3rd aspect (Figure 1).

Figure 2: Intra oral picture pre-treatment.
Intra orally diffuse, irregularly shaped mixed reddish white lesion seen over the buccal, labial mucosa, tongue, and hard and soft palate junction measuring about 1 x 2 cm to 1 x 0.5 cm in size. Surrounded by erythematous borders with pseudomembranous slough present centrally (Figure 2). On palpation, these lesions were tender, and soft in consistency. No pus discharge or blood, also Nikolsky’s sign was negative. Based on clinical history and examination provisional diagnosis of erythema multiforme was made. And mucositis, fixed drug eruption was considered as a differential diagnosis. After this investigations were conducted including CBC, RBS, and LFT in which no abnormality was found. Later the patient was prescribed topical steroid (triamcinolone 0.1%), bezadiamine oral rinse, antioxidants and systemic steroid (prednisone 10 mg per day) for 1 week. After 1 week of follow-up marked reduction was seen over the mucosal and lip lesion with no history of recurrence. The steroid dose was tapered after 14 days until the complete healing of the mucosal lesion was achieved (Figure 3).
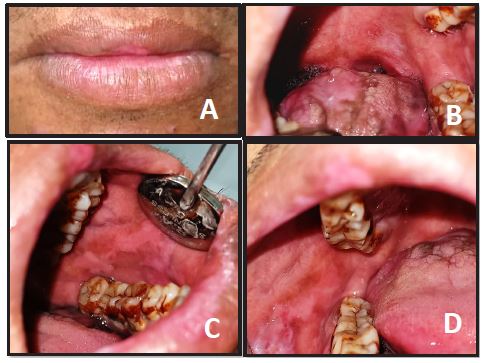
Figure 3: Post-treatment pictures.
Discussion
Erythema Multiforme (EM) is a severe, self-limiting, and recurrent mucocutaneous disorder that arises due to an allergic host response to an antigenic challenge, resulting in a distinct reaction pattern [3]. It may mimic various conditions, such as Stevens-Johnson syndrome, fixed drug eruptions, bullous pemphigoid, paraneoplastic pemphigoid, Sweet’s syndrome, Rowell’s syndrome, polymorphous light eruption, and cutaneous small-vessel vasculitis [4]. EM predominantly affects young adults, typically presenting between the second and fifth decades of life. Mucosal lesions occur in roughly 25-60% of EM cases [5]. Mucosal involvement usually coincides with skin involvement, but it can also precede or follow the appearance of skin lesions for several days. In rare cases, patients may exhibit mucosal lesions without any accompanying skin involvement. In our case, the patient was presented with oral lesions without skin lesions [6].
Almost 70% of patients with EM exhibit oral manifestations, such as swollen, cracked, and crusted lips, bleeding, and intraoral lesions on the non-keratinized mucosa, particularly in the anterior parts of the mouth. The appearance of diffuse, widespread macules that progress to blisters and ulcers makes it clinically challenging to distinguish EM from other vesiculobullous disorders [7]. Mechanisms underlying the pathogenesis of EM have been elucidated through analytical studies of HSV-associated EM. It is believed to result from a cell-mediated immune response against viral antigen-positive cells containing the HSV DNA polymerase gene (pol). Mononuclear cells, such as macrophages and CD34+ Langerhans cell progenitors, phagocytose the virus in peripheral blood, which possesses the skin-homing receptor cutaneous lymphocyte antigen. The engulfed HSV DNA is then transported to the epidermis, where the fragmented viral DNA is transferred to keratinocytes. Upregulation of E-cadherin expression enhances the binding of HSV-containing Langerhans cells to endothelial cells. Additionally, the upregulation of adhesion molecules on endothelial cells contributes to the inflammatory response [3]. EM can be divided into two primary types based on the severity and clinical presentation of the lesions EM minor and EM major.
In EM minor, skin lesions generally appear as macules or erythematous papules that evolve into classic target or iris lesions arranged symmetrically and occasionally develop into bullae. “Typical targets” are defined as individual lesions less than 3 cm in diameter, featuring a regular round shape, a well-defined border, and two concentric palpable oedematous rings that are paler than the central disc. Conversely, “raised atypical targets” are more frequently seen in severe EM major and Stevens-Johnson syndrome. These lesions resemble typical targets but are palpable [7], EM minor typically affects a single mucous membrane, most often the oral mucosa [5]. It is characterized by symmetrically distributed rashes on the extensor surfaces of the arms and legs. These rashes usually manifest as “iris” or “target” lesions or bullae on the extremities and may be accompanied by itching [8]. In EM major, the severity of lesions is greater, often involving multiple mucous membranes such as the oral cavity, genitalia, eyes (ocular), larynx, or oesophagus, either individually or in combination [5].
Stevens-Johnson Syndrome (SJS) is more severe than EM major, causing extensive lesions affecting the skin, oral cavity, eyes, pharynx, larynx, esophagus, and genitals. It may also present with symptoms like flu-like symptoms, fever, sore throat, headache, joint pain (arthralgias), muscle pain (myalgias), pneumonia, nephritis (kidney inflammation), or myocarditis (heart inflammation). Ocular changes, such as dry eyes and adhesions between the eyelid and eyeball (symblepharon), similar to those in mucous membrane pemphigoid, can occur with SJS. In some cases, SJS can result in dryness of the eyes and mouth (sicca syndrome) or progress to Sjögren’s syndrome [9]. Diagnosing EM relies predominantly on clinical history and examination findings rather than specific diagnostic tests. Important aspects of the clinical history include: (1) a sudden onset with a self-limiting or recurrent course, (2) symptoms suggestive of related infections like HSV, and (3) recent use of new medications. Clinical clues aiding diagnosis include the presence of characteristic target lesions, raised atypical papules, mucosal involvement, or a combination of these features [10].
Treatment starts with identifying the triggering agent; discontinuation is recommended if a drug was initiated within the last 7-21 days. Because of its viral cause, acyclovir is usually prescribed at 400 mg four times daily for six months. Alternatively, continuous prophylactic use of valacyclovir at 500 mg twice daily may be considered. Palliative measures include applying topical analgesics, using viscous lidocaine rinses, employing soothing mouth rinses, and adhering to a bland, soft diet while avoiding acidic and spicy foods. Supportive care should include liquid diets, intravenous fluids, electrolyte management, and nutritional support [11].
Conclusion
The clinical presentation of Erythema Multiforme (EM) is complicated and is impacted by immunological responses to a variety of stimuli, including infections such as the herpes simplex virus and certain medicines. Its characteristic target lesions and possible involvement of the mucosa highlight the urgency of early diagnosis and treatment. In addition to providing supportive care and corticosteroids for symptomatic relief, treatment approaches concentrate on locating and eliminating triggers. Even though EM presents dramatically, most instances resolve on their own, and the prognosis is usually positive. We continue to improve our knowledge and treatment of this difficult illness by ongoing research into its aetiology and the best therapy strategies.
References
- Krishnankutty K, Chaudhuri K, Ashok L. Erythema multiforme: A case series and review of literature. Open Access J Trans Med Res. 2018; 2(4): 124-30
- Nazir A, Ali K. Drug induced erythema multiforme-oral variant: A case report. Oral Maxillofac Surg Cases. 2022; 8(1): 100241.
- Rashmitha A, Gotoor SG, Muppirala S, Raju DR. Erythema multiforme: A case report. J Indian Acad Oral Med Radiol. 2017; 29(2): 153-155.
- Su JR, Haber P, Ng CS, Marquez PL, Dores GM, Perez-Vilar S, Cano MV. Erythema multiforme, Stevens Johnson syndrome, and toxic epidermal necrolysis reported after vaccination. Vaccine 2020; 38(7): 1746-52. 1999-2017.
- Huff JC, Weston WL, Tonnesen MG. Erythema multiforme: A critical review of characteristics, diagnostic criteria, and causes. J Am Acad Dermatol. 1983; 8: 763-775.
- Wetter DA, Davis MD. Recurrent erythema multiforme: clinical characteristics, etiologic associations, and treatment in a series of 48 patients at Mayo Clinic, 2000-2007. J Am Acad Dermatol. 2010; 62: 45-53.
- Scully C, Bagan J V. Oral mucosal diseases: erythema multiforme. Br J of Oral and Maxillofac Surg. 2008; 46: 90-95.
- Kaur H, Kaur M. Drug-induced erythema multiforme: A case report. Int J Oral Health Dent. 2018; 4(3): 175-179.
- de Roux Serratrice C, Serratrice J, Granel B, et al. Syndrome de Stevens-Johnson suivi d’un syndrome de Gougerot-Sjogren. [Stevens-Johnson syndrome followed by Gougerot-Sjogren syndrome]. Presse Med. 2001; 30: 531-2.
- Simbli MA. Erythema multiforme: Challenging diagnosis for internist. J Clin Case Rep. 2013; 3(7): 285-88.
- Vihan A, Patil RG, Murari A, Debnath S, Khan A. Drug-induced erythema multiforme: Case report. IJDSCR. 2024; 6(3): 69-74.
