
Open Access, Volume 10
Case report: FDAL causing bilateral tarsal tunnel syndrome
Soham Ganguly1; James Cusack2; Akash Ganguly2
1Medical School, University College London, 74 Huntley Street, London WC1E 6DE, UK.
2Department of Radiology, Warrington & Halton Hospitals, NHS Foundation Trust, Warrington Hospital, Lovely Lane, Warrington, Cheshire WA5 1QG, UK.
Akash Ganguly
Department of Radiology, Warrington & Halton Hospitals, NHS Foundation Trust, Warrington Hospital,
Lovely Lane, Warrington, Cheshire WA5 1QG, UK.
Email: drakash_ganguly@yahoo.co.uk
Received : August 08, 2024,
Accepted : August 27, 2024
Published : August 30, 2024,
Archived : www.jclinmedcasereports.com
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Ganguly A (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Ganguly S, Cusack J, Ganguly A. Case report: FDAL causing bilateral tarsal tunnel syndrome. Open J Clin Med Case Rep. 2024; 2279.
Clinical History and Imaging
A 49-year-old woman presented to orthopaedic clinic with a two-year history of pain at the back of both of her heels. She started doing a lot of walking during the Covid-19 lockdown. The symptoms were intermittent and are worse on weight bearing whilst walking. The pain was localised to the posterior medial aspect of the heels. There was no history of trauma.
On examination, the patient walked with a normal gait. There was a good range of ankle and subtalar movements, and the heel was in the neutral position. She was tender over the posterior medial aspect of the heel distal to the insertion of the tendo achilles. The tendo achilles was non-tender. There was some mild tenderness over the superficial bursa but none over the retrocalcaneal bursa. There is no tenderness over the plantar fascia.
X-rays were done of both ankles at this point. Due to the unremarkable findings on the x-rays MRI scans of both ankles was requested.
MRI of the left ankle showed borderline thickening of the Achilles tendon measuring 6mm with minor high signal in the Kager’s fat pad. There was a prominent FDAL (Flexor Digitorum Accessorius Longus) accessory muscle in the tarsal tunnel resulting in crowding on the neurovascular bundle (Figure 1). The rest of the tendons and ligaments of the joint looked unremarkable.
MRI of the right ankle also showed an accessory FDAL muscle with crowding of the tarsal tunnel (Figure 2). The rest of the tendons and ligaments around the ankle joint looked unremarkable.
The cause of her pain was the prominent FDAL accessory muscle in the tarsal tunnel which was causing crowding impinging upon the neurovascular bundle. The patient was advised to avoid wearing ankle socks or any sandals that may cause compression or tightness in the region. The patient was not keen for tarsal tunnel decompression so had conservative management with massaging of the area.
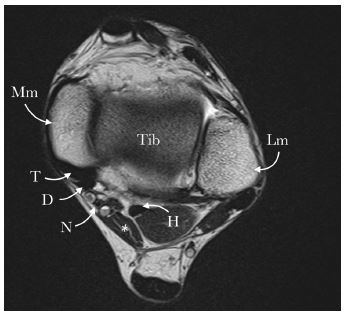
Figure 1: Axial T2 W image of the left ankle showing an FDAL muscle (*) with crowding of the tarsal tunnel.
Mm: Medical malleolus; Lm: Lateral malleolus; Tib: Tibia; T: Tibialis posterior tendon; D: Flexor digitorum longus tendon; N: neurovascular bundle of posterior tibial vessels and tibial nerve; H: Flexor hallicus longus tendon
Mm: Medical malleolus; Lm: Lateral malleolus; Tib: Tibia; T: Tibialis posterior tendon; D: Flexor digitorum longus tendon; N: neurovascular bundle of posterior tibial vessels and tibial nerve; H: Flexor hallicus longus tendon
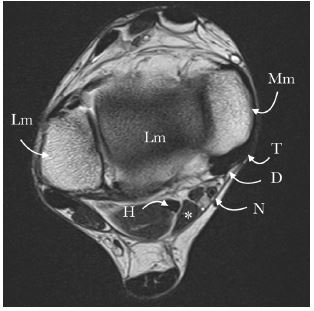
Figure 2: Axial T2 W image of the right ankle showing an FDAL muscle (*) with crowding of the tarsal tunnel
Mm: Medical malleolus; Lm: Lateral malleolus; Tib: Tibia; T: Tibialis posterior tendon; D: Flexor digitorum longus tendon; N: Neurovascular bundle of posterior tibial vessels and tibial nerve; H: Flexor hallicus longus tendon
Mm: Medical malleolus; Lm: Lateral malleolus; Tib: Tibia; T: Tibialis posterior tendon; D: Flexor digitorum longus tendon; N: Neurovascular bundle of posterior tibial vessels and tibial nerve; H: Flexor hallicus longus tendon
Discussion
The tarsal tunnel is located postero-medially on the ankle. It is bordered by the calcaneus, talus and medial aspect of the tibia on the floor [1]. The roof is formed by the flexor retinaculum, which spans between the medial malleolus and the medial tubercle of the calcaneus. It contains (anteriorly to posteriorly) the tibialis posterior tendon, the flexor digitorum longus tendon, the posterior tibial artery and vein, the tibial nerve and the flexor hallicus longus tendon.
The FDAL muscle is the most common accessory muscle in the posterior compartment of the ankle, and the second most common accessory in the ankle area in general [2]. It has a reported incidence of 2-8% in the lower limbs [3]. It can originate from a number of structures in the lower limb, including the tibia, the fibula, any muscles in the deep posterior leg or the posterior intermuscular septum [2].
FDAL has been described to either have a single or a double head which usually shows a fleshy, tendinous or aponeurotic appearance as it courses from the leg down through the tarsal tunnel to its insertion in the Flexor Digitorum Longus (FDL) and/or the quadratus plantae [4].
The tarsal tunnel runs behind the medial malleolus inferiorly. The posterior tibial nerve passes through this tunnel between the FDL and flexor hallicus longus muscles [5]. Compression of this nerve leads to tarsal tunnel syndrome, and this is characterised by pain, tingling or numbness in the foot [6]. MRI is a modality of imaging that can depict the bones, soft tissues and boundaries of the tarsal tunnel.
Management of patients with tarsal tunnel syndrome remains challenging. Some patients are managed conservatively with physiotherapy and analgesia such as non-steroidal anti-inflammatory drugs [7]. If conservative management does not work, surgical decompression can be considered. MRI is useful in these cases to identify FDAL and to exclude other causes of ankle pain (ibid).
Conclusion
The FDAL muscle is an accessory muscle with an incidence of 2-8%. MRI scans show a fleshy appearance through the tarsal tunnel. Recognition of FDAL on MRI plays an important part of diagnosing tarsal tunnel syndrome and implementing appropriate management. This case showed a case where FDAL was seen bilaterally and caused bilateral tarsal tunnel syndrome.
References
- Jones O. The Tarsal Tunnel. Teach Me Anatomy. 2021. Available from: https://teachmeanatomy.info/lower-limb/areas/tarsal-tunnel/
- Shin JH, Shim JC, Lee KE, Kim HK, Lee GJ, et al. The MRI findings of flexor digitorum Accessorius Longus Muscle: A case report. Investigative Magnetic Resonance Imaging. 2016; 20(2): 123-6.
- Pellis Z, Bandak MC, Bolden A, Zdilla M, Lambert HW. Discovery of a flexor digitorum accessorius longus (FDAL) muscle - implications for tarsal tunnel syndrome. The FASEB Journal. 2021; 35(S1).
- Sarrafian SK, Kelikian AS. Myology. In: Sarrafian’s Anatomy of the Foot and Ankle: Descriptive, Topographic, FunctionalM. Philadelphia, PA: Lippincott Williams & Wilkins. 2011; 223-92.
- Samaras D. Tarsal tunnel syndrome caused by a flexor digitorum accessorius longus muscle: A case report and review of the literature. Journal of Foot and Ankle Research. 2011; 4(S1): 484-7.
- Tarsal tunnel syndrome. Tarsal Tunnel Syndrome. | Johns Hopkins Medicine. 2021. Available from: https://www.hopkinsmedicine.org/health/conditions-and-diseases/tarsal-tunnel-syndrome#:~:text=Tarsal%20tunnel%20syndrome%20(TTS)%20is,or%20numbness%20in%20the%20foot.
- Kiel J, Kaiser K. Tarsal Tunnel Syndrome. StatPearls Publishing, Treasure Island (FL). 2018.
