
Open Access, Volume 10
Resurgence of measles in Morocco in 2024: Experience of the Mohamed V Military Hospital
Elbenaissi*; N Zniber; S Elkochri; Y Aadi; I Roufik; A Regad; M Elqatni; M Tagajdid; H Elannaz; A Laraqui; B Elmchichi; N Touil; K Ennibi; I Lahlou Amine; R Abi
Department of Virology, Mohammed V Military Teaching Hospital, Mohammed V University, Morocco.
Y Elbenaissi
Department of Virology, Mohammed V Military Teaching Hospital, Mohammed V University, Morocco.
Email: bnaissiyassine@gmail.com
Received : August 04, 2024,
Accepted : August 26, 2024
Published : August 30, 2024,
Archived : www.jclinmedcasereports.com
Abstract
In a global context marked by a surge in measles epidemics and its spread across various regions (Europe, Africa, and the United States), Morocco has recorded an increased case, challenging existing control measures. This study aimed to determine the epidemiological, clinical, virological, and evolutionary aspects of hospitalized measles cases in our facility. A cross-sectional study was conducted between March and June 2024. All measles cases were confirmed through various serological and biological techniques. During the study period, seven measles cases were admitted to our facility, with a male predominance (5/7, or 71.4%) and an average age of 37 years. Measles vaccination was confirmed in only one person, while four patients (57.1%) were unvaccinated, and two (28.6%) had an unknown vaccination status. Clinically, rash and fever were consistent and often associated with oculo-nasal catarrh, respiratory issues, and digestive disturbances. All patients tested positive for IgM antibodies using the ELISA test, and the detection of viral RNA by RT-PCR in respiratory (nasal and oropharyngeal) and saliva samples confirmed the diagnosis across all samples. Genetic analysis revealed that six MeV isolates belonged to genotype B3, with one genotype D8. Viral culture on the Vero/dog SLAM cell line demonstrated morphological changes (syncytia) due to the typical Cytopathic Effect (CPE) of the measles virus produced by viral replication in cell culture. The average duration of clinical symptoms was eleven days under symptomatic treatment, with no complications reported during the patient’s hospital stay. The observed resurgence of measles cases in Morocco underscores the importance of strengthening epidemiological surveillance and vaccination campaigns to limit the virus’s spread.
Keywords: Measles; Clinical; Genetic epidemiology; Morocco.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Elbenaissi Y (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Elbenaissi Y, Zniber N, Elkochri S, Aadi Y, Roufik I, Regad A, Elqatni M, et al. Resurgence of measles in Morocco in 2024: Experience of the Mohamed V Military Hospital. Open J Clin Med Case Rep. 2024; 2778.
Introduction
Thanks to national vaccination activities within the framework of the national immunization program, Morocco has seen a significant decrease in measles cases, with an incidence of less than 1 per 1 million inhabitants and vaccination coverage exceeding 95% [1]. However, at the beginning of 2024, in a global context marked by a surge in measles epidemics and its spread across various regions (Europe, Africa, and the United States), Morocco recorded an increase in measles cases [2].
Our work aimed to determine the epidemiological, clinical, virological, and evolutionary aspects of measles cases hospitalized at the virology, infectious, and tropical diseases center of the Mohammed V Military Teaching Hospital.
Patients and Methods
This is a descriptive cross-sectional study conducted among measles patients admitted to our facility from March 22, 2024, to June 22, 2024. The case definition of measles used in our research is that of the World Health Organization (WHO), which defines a measles case as any individual presenting with a maculopapular erythematous rash lasting at least three days, accompanied by a fever above 38.5°C, and one of the following three signs: cough, rhinorrhea, or conjunctivitis [3].
Biological confirmation was performed by combining various serological and molecular biology techniques. All our patients underwent a thorough clinical and paraclinical examination to search for complications. Data entry and analysis were performed using Jamovi software.
Results
During the study period, seven measles cases were admitted to our facility. All cases originated from the urban area of the Rabat-Sale-Kenitra region, with a predominance of males (5/7 or 71.4%) and a male-to-female sex ratio of 0.71. The average age of the patients was 37 years, with an age range of 32 to 48 years. Vaccination against measles was confirmed in only one person, while four patients (57.1%) were unvaccinated, and two patients (28.6%) had an undetermined vaccination status. A history of familial transmission was reported in 28.6% of cases, despite 57.1% of the patients having school-aged children. Clinically, skin rash (Figure 1) and fever were constant findings, often accompanied by ocular-nasal catarrh, respiratory disorders, and digestive issues. None of our patients presented with respiratory or neurological disorders at admission. The pathognomonic Koplik spots were observed in only one patient. Initial biological assessments revealed profound lymphopenia in 85.7% of the cases and a marked inflammatory syndrome in all participants, with an average C-Reactive Protein (CRP) level of 48 mg/l. The viral infection was also associated with thrombocytopenia in 43% of the patients and hepatic cytolysis in 57% of our patients. Thoracic imaging did not reveal any lesions suggestive of bronchopneumonia in any of our patients (Table 1).

Figure 1: Characteristic skin rash of measles observed in one of our patients.
Table 1: Biological, clinical, and epidemiological aspects of the measles case.
| Population size | Percentage (%) | ||
|---|---|---|---|
Age |
- Mean - Standard deviation |
37 years 6 years |
|
Sex |
- Male - Female |
5 2 |
71.4 28.6 |
Vaccinal status |
- Vaccinated - Unvaccinated - Unknown |
1 4 2 |
14.3 57.1 28.6 |
| Familial transmission | 2 | 28.6 | |
| Contact with children | 4 | 57.1 | |
Clinical manifestations |
- Skin rash - Ocular-nasal catarrh - Koplik spot - Digestive disorders - Respiratory disorders - Neurological disorders |
7 4 1 2 3 0 |
100 57.1 14.3 28.6 42.9 0 |
Hemogram |
- Severe lymphocytopenia ( < 700 elements/mm3) - Thrombocytopenia(< 150000 element/mm3) |
6 3 |
85.7 42.9 |
| Inflammatory biomarkers | - CRP (mean)(mg/l) - Ferritin (mean) (mg/l) |
48 460 |
|
| Hepatic biomarkers | - Hepatic cytolysis (ALAT > x2 N) - Cholestatis (BT> 10 umol/l) |
4 1 |
57.1 14.3 |
| Mean hospital length of stay (days) | 6 |
Table 2: Results of serological and molecular testing of patients in our series.
| Patient N° | IgMantibody | IgGantibody | RT-PCR | Genotype |
|---|---|---|---|---|
| 1 | Positive | Negative | Positive | D8 |
| 2 | Positive | Negative | Positive | B3 |
| 3 | Positive | Negative | Positive | B3 |
| 4 | Positive | Negative | Positive | B3 |
| 5 | Positive | Negative | Positive | B3 |
| 6 | Positive | Negative | Positive | B3 |
| 7 | Positive | Negative | Positive | B3 |
The confirmation of the diagnosis was performed using viral serology for measles on a peripheral blood sample to detect markers of an immune response against this virus (IgM/IgG) and an RT-PCR to detect viral RNA in respiratory (nasopharyngeal and oropharyngeal) and salivary samples (Table 2).
The confirmation of the diagnosis was performed using viral serology for measles on a peripheral blood sample to detect markers of an immune response against this virus (IgM/IgG) and an RT-PCR to detect viral RNA in respiratory (nasopharyngeal and oropharyngeal) and salivary samples (Table 2).
The isolation of the measles virus in culture was performed using the Vero/dogSLAM cell line, which is permissive, safe, and easy to use for the growth of the measles virus. This cell line was developed by transfecting the Vero cell line with a plasmid encoding the gene for the canine Signaling Lymphocyte Activation molecule (dogSLAM). The DogSLAM receptor has been identified as the cellular receptor for the measles virus. The treated sample was inoculated with gentamicin on a pre-established Vero/dogSLAM cell monolayer at 85-95% confluence. After incubation at 37°C, daily microscopic observation of the cells allowed for the detection of morphological changes in the Vero/dogSLAM cells, or the Cytopathic Effect (CPE), produced by the replication of the measles virus in cell culture. The typical CPE consists of the formation of syncytia, which appear as large multinucleated cells caused by the fusion of infected cells (Figure 2).
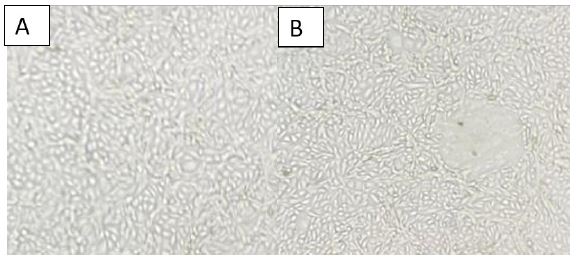
Figure 2: CPE of the Measles Virus on Vero/dogSLAM Cells
(A) Uninfected Vero/dogSLAM cell line, 100×
(B) Vero/dogSLAM cell line infected with the measles virus, showing syncytia formation after 72 hours of infection, 100×
(A) Uninfected Vero/dogSLAM cell line, 100×
(B) Vero/dogSLAM cell line infected with the measles virus, showing syncytia formation after 72 hours of infection, 100×
The average hospitalization duration was 6±2 days (range: 4-10 days). After symptomatic treatment (antipyretics, analgesics, antiseptic eye drops, antibiotics, and vitamin A therapy), no patients developed complications during their stay. Clinical symptoms lasted an average of 11 days from the onset of infection.
Discussion
Measles remains a significant public health issue globally, with approximately 9.7 million cases and over 140,000 deaths in 2018[1]. In Morocco, despite a vaccination coverage exceeding 95%, herd immunity has not been achieved due to the persistence of high-risk pockets (peri-urban areas, isolated rural localities) and the high transmissibility of the virus. This has led to epidemic resurgences, such as in 2013[1]. Currently, Morocco has recorded 7,869 measles cases (2,753 confirmed) and 19 deaths (case-fatality rate of 0.2%) across the 12 regions of the country, with an incidence rate of 21.1 per 100,000 inhabitants [4].
At the Center for Virology, Infectious, and Tropical Diseases, seven cases were hospitalized over four month, with a hospitalization incidence of 5.8%. All were adults, with an average age of 37 years and a sex ratio of 0.71. These findings are similar to those reported in other studies [5,6]. 81.7% of our patients were unvaccinated or had an unknown vaccination status. This high incidence in our study can be attributed to the late introduction of the measles vaccine in Morocco in 1987, with vaccination coverage exceeding 90% only achieved by the beginning of 1995 [1,7]. Other authors have also noted a two- to three-fold higher rate among unvaccinated individuals [8,9].
Clinically, fever and mucocutaneous rashes were often associated with pneumonia (42.9%) and digestive disorders (28.6%). These results are consistent with the literature [6,10]. The average hospitalization duration was 6 days, with an average symptom duration of 11 days, similar to findings from a 2020 study by Paraskev in Greece [6].
The most appropriate sample to assess the immune status of contacts is serum. It is essential to collect serum samples at the correct time relative to rash onset, as they may still be undetectable for IgM within three days of rash onset [11].
A buccal swab should be collected by rubbing the swab along the gum and then on the tongue. Throat or nasopharyngeal buccal swabs can be used for PCR if collected within six days of rash onset. A negative PCR result does not exclude a measles diagnosis, especially whithout cellular RNA control to verify sample quality [11].
Measles virus genotyping is an essential tool in epidemiological surveillance. It identifies the origin of the virus, and its transmission pathways, and evaluates vaccination programs. Given the importance of genotyping in the measles elimination program, a rapid technique has been developed. This technique identifies genotypes by real-time PCR, with different genotypes distinguished by their melting Temperature (Tm). This method is an effective alternative for investigating measles outbreaks in countries in the elimination phase. Measles virus strains isolated during the 2024 season were identified by real-time PCR and confirmed by sequencing the H and N genes. This study showed that the indigenous strain (B3) remains dominant, while the imported genotype (D8) from Europe is circulating in Morocco [12].
Conclusion
The Ministry of Public Health, through regional directorates, has taken a series of measures to strengthen epidemiological surveillance and vaccination campaigns to limit the spread of the virus. The vaccination schedule in Morocco includes two doses against measles at nine and eighteen months. If symptoms suggestive of the disease appear, the Ministry recommends visiting the nearest health center for appropriate treatment.The Ministry of Public Health, through regional directorates, has taken a series of measures to strengthen epidemiological surveillance and vaccination campaigns to limit the spread of the virus. The vaccination schedule in Morocco includes two doses against measles at nine and eighteen months. If symptoms suggestive of the disease appear, the Ministry recommends visiting the nearest health center for appropriate treatment.
References
- Bulletin 2022 d’epidemiologie et de santé publique. 2022.
- I Cherkaoui, A Fakhreddine, K El Massaoudi, et al. Zidouh. Investigation d’une épidémie de rougeole dans la localité de Kouf, province de Tétouan, Maroc. Eastern Mediterranean Health Journal. 2024; 30.
- Organisation mondiale de la sante´ (OMS). Traitement de la rougeole chez l’enfant. 1998 WHO/EPI/LHIS.97.02.
- P.GEROME. Africa CDC Weekly Event Based Surveillance Report. 2024.
- E. BenChetrit, et al. Measles-related hospitalizations and associated complications in Jerusalem, 2018-2019, Clin. Microbiol. Infect. 2019.
- C Paraskevi, et al. Clinical characteristics and outcomes of measles outbreak in adults: A multicenter retrospective observational study of 93 hospitalized adults in Greece. Journal of Clinical Virology. 2020; 131: 104608.
- N.Bouazzaoui. Évolution of the Vaccination Timetable in Morocco. Bull. Acad. Natle Méd. 2006; 190: 1017-1033.
- www.who.int/europe/fr/news/item/14-12-2023-a-30-fold-eise-of-measles-cases-in-2023-in-the-who-european-region-warramts-urgent-action.
- J.Marie Manus. L’Europe confrontée à une recrudescence de la rougeole. Revue Francophone des Laboratoires, 2024-03-01. 2024; 560: 6-6.
- J.M Hübschen. Measles. Lancet. 2022; 399: 678-90.
- National measles guidelines. 2024.
- A.alla, D.Waku-Kouomou. Génotypage du virus de la rougeole par PCR en temps réel: Cas des souches virales isolées au Maroc pendant la saison 2004-2005 LES TECHNOLOGIES DE LABORATOIRE. 2007.
