
Open Access, Volume 10
Laryngeal involvement in pulmonary tuberculosis: A case report
Kristian Bugeja*; Michela Manfre; Luke Bonello; Alexandra Betts; Carmel Borg
Mater Dei Hospital, Malta.
Kristian Bugeja
Mater Dei Hospital, Malta.
Email: kristianbugeja.md@gmail.com
Received : July 24, 2024,
Accepted : August 22, 2024
Published : August 30, 2024,
Archived : www.jclinmedcasereports.com
Abstract
This case report documents the presentation, diagnosis, and management of a 31-year-old female with pulmonary tuberculosis with laryngeal involvement. The patient presented with severe dysphonia and hoarseness unresponsive to antifungal treatment. Initial examination revealed gross granulomatous disease throughout the larynx. A biopsy confirmed necrotizing granulomatous inflammation. Imaging studies were consistent with pulmonary tuberculosis. The patient was treated with a standard anti-tuberculosis regimen, and after a brief period of hospitalization, was discharged to continue treatment at home. This case highlights the complexities of diagnosing and managing laryngeal tuberculosis, underscoring the importance of thorough evaluation and multidisciplinary care.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Bugeja K (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Bugeja K, Manfre M, Bonello L, Betts A, Borg C. Laryngeal involvement in pulmonary tuberculosis: A case report. Open J Clin Med Case Rep. 2024; 2277.
Case Report
In January 2024, a 31-year-old female, presented with a two-week history of severe dysphonia and hoarseness, unresponsive to antifungal therapy. On examination, flexible nasoendoscopy revealed extensive lesions characterized by irregular, inflamed, and nodular tissue extending from the epiglottis to the anterior commissure and down to the vocal cords.
A direct laryngoscopy with biopsy was performed in the following month, and biopsies were taken from the left false vocal cord, anterior commissure, left aryepiglottic fold and the laryngeal aspect of the epiglottis. In several of these biopsies necrotizing granulomatous inflammation with suppuration was identified, characterized by aggregates of epithelioid histiocytes and occasional Langhans type multinucleated giant cells surrounding geographic areas of necrosis (Figure 1). Neutrophilic infiltration of the underlying cartilage was seen in places. No acid-fast bacilli were identified with a Ziehl-Neelsen stain. PAS and Grocott stains were negative for fungal hyphae. Shavings from these biopsies were also submitted for PCR, which detected Mycobacterium tuberculosis.
The patient was admitted to the hospital with a diagnosis of pulmonary tuberculosis with laryngeal involvement. A CT thorax performed, showed findings consistent with radiologically established pulmonary tuberculosis with upper zonal predominance (Figure 2). A CT neck on the same day revealed mild thickening of the epiglottis, particularly on its cranial aspect, and mild superficial enhancement at the level of the supraglottis (Figure 3).
Microbiological investigations included three sputum cultures, which showed no growth. However, Mycobacteria PCR confirmed the presence of M. tuberculosis complex, sensitive to Rifampicin and Isoniazid. Direct Ziehl-Neelsen staining of sputum revealed Grade 3+ acid-fast bacilli. Beta-D-glucan and galactomannan tests were normal.
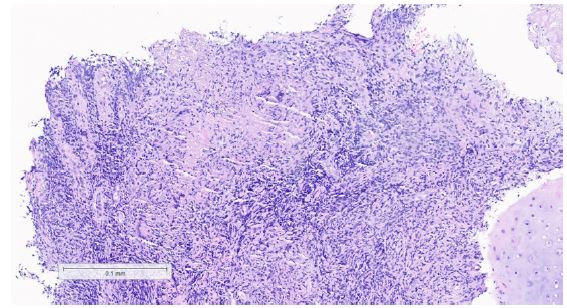
Figure 1: Histological section from a biopsy of the laryngeal aspect of the epiglottis showing necrotising granulomatous inflammation with suppuration.
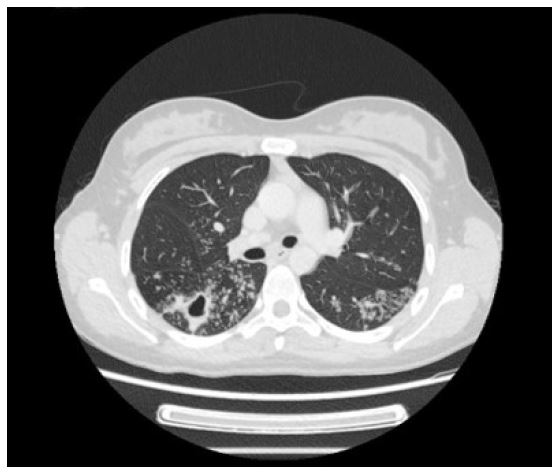
Figure 2: CT Thorax showing tree-in-bud segments in the apical segments of bilateral lower lobes, along with a cavitating lesion in the right lung.
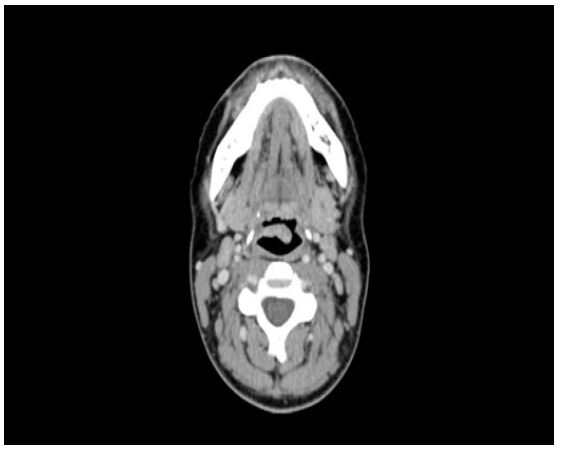
Figure 3: CT Neck demonstrating moderate swelling of the epiglottis, more pronounced on the left side than the right.
The patient was started on a regimen of Rifinah, Pyrazinamide, Ethambutol and Pyridoxine. The patient was discharged after completing ten days of anti-TB treatment in the hospital. Given her living situation, she was deemed able to continue treatment at home. The discharge plan included the continuation of anti-TB medications with Pyridoxine, and isolation for another ten days. She was followed up by both ENT and infectious disease over the following weeks.
This case illustrates the need for comprehensive evaluation and multidisciplinary management in cases of pulmonary tuberculosis with laryngeal involvement. Her positive initial response to treatment and detailed follow-up plan highlight the importance of continued care and monitoring in managing complex tuberculosis cases.
Discussion/Literature Review
Laryngeal Tuberculosis (LTB) is a rare manifestation of Tuberculosis (TB), accounting for less than 2% of extrapulmonary TB cases. However, it remains the most frequent granulomatous disease of the larynx. The incidence of LTB among patients with pulmonary TB varies significantly, ranging from 0.08% to 5.1%, likely due to underdiagnosis from the lack of routine otorhinolaryngologic evaluations in TB patient [1,2]. In terms of epidemiology, LTB is more common in adults, with a slight male predominance noted in some studies. The incidence appears higher in populations with higher rates of pulmonary TB and those with conditions that compromise the immune system, such as HIV infection [2].
LTB can manifest through various symptoms, with voice impairment being the most common. Symptoms can range from hoarseness and dysphonia to severe cases presenting with stridor or airway obstruction. The diagnosis is often delayed because LTB can mimic other laryngeal diseases, such as malignancies or other chronic granulomatous conditions like sarcoidosis or Wegener's granulomatosis [2,3].
Diagnosis of LTB is confirmed through a combination of imaging studies, histopathologic examination, and microbiological analysis. Chest X-rays and CT scans typically reveal concomitant pulmonary TB. Direct laryngoscopy with biopsy is crucial for obtaining tissue samples for definitive diagnosis, identifying necrotizing granulomatous inflammation typical of TB [3,4].
Risk factors for LTB include immunosuppression, HIV infection, and a history of pulmonary TB. Smoking and alcohol consumption are also associated with higher risks of developing LTB [1,4]. Laryngeal TB primarily affects adults, with a slight male predominance noted in some studies [2].
LTB is often secondary to pulmonary TB, resulting from bronchogenic spread of Mycobacterium tuberculosis. Less commonly, it can occur as a primary infection through direct seeding of the larynx. LTB can affect any part of the larynx, with the true vocal folds, false vocal folds, and epiglottis being the most commonly involved sites [3,5].
The management of LTB involves the standard Anti-Tuberculosis Therapy (ATT), similar to pulmonary TB. A combination of isoniazid, rifampicin, pyrazinamide, and ethambutol is typically administered over a 6-9 month period. Treatment success rates are high, but early diagnosis is essential to prevent complications such as airway obstruction and to reduce transmission risk [3].
The presented case of a 31-year-old female with LTB underscores the complexity of diagnosing and managing this rare form of TB. Despite initial misdiagnosis and treatment with antifungals, the thorough evaluation including imaging and biopsy eventually confirmed the diagnosis, allowing for appropriate ATT and successful patient recovery [4].
LTB remains a diagnostic challenge due to its rarity and nonspecific presentation. Enhanced awareness and comprehensive diagnostic protocols are essential for early identification and management of this condition. This case highlights the importance of considering LTB in patients with laryngeal symptoms and a history of TB, advocating for multidisciplinary approaches in management [3,5].
By understanding the epidemiology, clinical features, and management strategies of LTB, healthcare providers can improve outcomes for patients affected by this rare but significant manifestation of TB [1,4-9].
Abbreviations: PCR: Polymerase Chain Reaction; PAS: Periodic Acid-Schiff; CT: Computed Tomography; ENT: Ear, Nose, And Throat TB: Tuberculosis; M. Tuberculosis: Mycobacterium Tuberculosis; LTB: Laryngeal Tuberculosis; HIV: Human Immunodeficiency Virus; ATT: Anti-Tuberculosis Therapy; CXR: Chest X-Ray.
References
- Rizzo PB, Da Mosto MC, Clari M, Scotton PG, Vaglia A, et al. Laryngeal Tuberculosis: an often forgotten diagnosis. International Journal of Infectious Diseases. 2003; 7(2): 129-131.
- Shin JE, Nam SY, Yoo SJ, Kim SY. Changing trends in clinical manifestations of laryngeal Tuberculosis. Laryngoscope. 2000; 110(11): 1950-1953.
- Lodha JV, Sharma A, Virmani N, Bihani A, Dabholkar JP. Secondary laryngeal Tuberculosis revisited. Lung India. 2015; 32(5): 462-464.
- Harney M, Hone S, Timon C, Donnelly M. Laryngeal Tuberculosis: an important diagnosis. Journal of Laryngology & Otology. 2000; 114(11): 878-880.
- Lynrah KG, Tiewsoh I, Marbaniang E, Barman B, Synrem E, et al. Laryngeal Tuberculosis not uncommon in the Present era. Journal of Tuberculosis and Therapy. 2018; 3: 118.
- Guan LS, Jun TK, Azman M, Baki MM. Primary Laryngeal Tuberculosis Manifesting as Irregular Vocal Fold Lesion. Turkish Archives of Otorhinolaryngology. 2022; 60(1): 47-52.
- Swain SK, Behera IC, Sahu MC. Primary laryngeal Tuberculosis: our experiences at a tertiary care teaching hospital in Eastern India. Journal of Voice. 2019; 33(6): 812e9-81214.
- Agarwal R, Gupta L, Singh M, Yashaswini N, Saxena A, et al. Primary laryngeal Tuberculosis: a series of 15 cases. Head and Neck Pathology. 2019; 13(3): 339-343.
- Huon LK, Fang TY. Primary laryngeal Tuberculosis. Journal of the Formosan Medical Association. 2011; 110(12): 792-793.
