
Open Access, Volume 10
Osteomyelitis of the mandible occurring during infliximab treatment of ankylosing spondylitis: A case report
Van Cauteren Laurent1*; Piccart Frederik1; Creytens David2; Bauters Wouter3; Ureel Matthias1; Coopman Renaat1
1Department of Oro-Maxillofacial, Plastic, Reconstructive and Aesthetic Surgery, Ghent University Hospital, Ghent, Belgium.
2Department of Pathology, Ghent University Hospital, Ghent, Belgium.
3Department of Radiology, Ghent University Hospital, Ghent, Belgium.
Van Cauteren Laurent
Department of Oro-Maxillofacial, Plastic, Reconstructive and Aesthetic Surgery, Ghent University Hospital, Ghent, Belgium.
ORCID ID: 0009-0002-5628-4295;
Email: Laurent.vancauteren@ugent.be
Received : July 24, 2024,
Accepted : August 20, 2024
Published : August 30, 2024,
Archived : www.jclinmedcasereports.com
Abstract
We present a case of a patient who received infliximab for ankylosing spondylitis who developed a left-sided mandibular osteomyelitis after a left mandibular molar extraction. After the formation of multiple abscesses and recurrent antibiotic treatments, the patient faced diagnostic challenges which led to a delayed diagnosis, eventually confirmed through MRI and bone probe sampling. MRI showed an altered signal intensity on T1- and T2-weighted images at the left mandibular corpus. Bone probe sampling identified Streptococcus mitis and Streptococcus parasanguinis as the causative microorganisms. This case report discusses the faced challenges in the diagnosis and management of mandibular osteomyelitis and highlights the importance of close follow-up after oral surgical interventions during immunomodulatory treatment. It contributes to the limited literature of the correlation between infliximab therapy and mandibular osteomyelitis.
Keywords: Infliximab; Osteomyelitis; TNF-α inhibitor; Complication tooth extraction.
Abbreviations: CT: Computed Tomography; ENT: Ear Nose Throat; MRI: Magnetic Resonance Imaging; OPAT: Outpatient Parenteral Antibiotic Therapy; OPT: Orthopantomograph; TNF-α: Tumor Necrosis Factor-alpha.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Laurent VC (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Laurent VC, Frederik P, David C, Wouter B, Matthias U, Renaat C. Osteomyelitis of the mandible occurring during infliximab treatment of ankylosing spondylitis-A case report. Open J Clin Med Case Rep. 2024; 2276.
Introduction
Infliximab, a monoclonal humanized antibody against Tumor Necrosis Factor-alpha (TNF-α), is used as a treatment in different inflammatory diseases, such as rheumatoid arthritis, ankylosing spondylitis and inflammatory bowel disease [1-3]. Infliximab is usually administered through intravenous infusion according to body weight at a dose of 3-5 mg/kg at weeks 0, 2, and 6. When used in maintenance therapy, infusions take place every 6-8 weeks [2,4]. Multiple adverse effects during infliximab treatment have been reported, including formation of lymphomas, diabetes mellitus and the development of non-melanoma skin cancers [2,3,5]. However, one of the less common reported side effects is osteomyelitis: A severe infectious disease that needs treatment and recognition, due to its potential to cause functional impairment or permanent disability in severe cases [6].
Osteomyelitis of the jaw is characterized by inflammation and infection of the jawbone and bone marrow. Various conditions such as oral surgery, cancer, traumatism, radiotherapy, bisphosphonate therapy and immune depression are known to be risk factors [7]. The incidence of osteomyelitis of the jaw decreased considerably the past five decades because of the progression in oral hygiene, the use of antibiotics and better access to medical care [6,7]. Despite all this, an average diagnostic delay of three years is reported in osteomyelitis of the jaws [6]. In craniofacial structures, osteomyelitis occurs more in the mandible than the maxilla [8]. This is due to the poor vascularization and the dense mandibular cortical bone, making the mandible more prone to damage and to infection after tooth extraction [9].
Case Presentation
A 56-year-old Caucasian female presented in a peripheral hospital with a significant left-sided soft tissue swelling and inflammation after a tooth extraction. Her medical history indicated a diagnosis of ankylosing spondylitis, for which she has been undergoing treatment with 6-weekly Remsima infusions (5 mg/kg infliximab IV) since June 1, 2021. Additionally, she has a history of coronary artery disease and underwent percutaneous coronary intervention of the left anterior descending artery in January 2023. The patient’s regular medication regimen includes Acetylsalicylic acid 80 mg 1 dd, Atorvastatin 20 mg 1 dd, Clopidogrel 75 mg 1 dd, Diclofenac retard 75 mg 2 dd, Olmesartan, Medoxomil/Amlodipine 20/5 mg 1 dd, Lormetazepam 1 mg 1dd, Macrogol 1 dd, Pantoprazole 40 mg 1 dd, Acetaminophen 1 g 3 dd, Clonazepam 2.5 mg/ml 9 drops dd, Escitalopram 10 mg 1 dd, Otilonium 40 mg 3 dd and Solifenacine 10 mg 1 dd.
A Computed Tomography-scan (CT-scan) was performed to assess the presence of pus in the fascial spaces of the perimandibular region on March 17, 2022. This scan revealed swollen cervical lymph nodes and a swollen left submandibular gland (Figure 1). In initial antibiotic treatment with amoxicillin and amoxicillin/clavulanic acid, there was no improvement observed. Subsequent drainage and culture revealed the isolation of Streptococcus constellatus, which was susceptible to ciprofloxacin and clindamycin.
Following the initial drainage procedures and antibiotic treatments, temporary relief was observed. However, recurrences of the infections persisted despite these interventions. Multiple further interventions were undertaken, including additional incision drainage procedures and the cancellation of infliximab administration due to the ongoing infection. Streptococcus constellatus persisted in the cultures. A surgical resection of the oral cutaneous fistula and remaining abscess was performed, which was followed by nine months of clinical stability. Infliximab was reintroduced five months into this stable period.
The nine-month period was ended by a low velocity, blunt force trauma against the left side of the neck, leading to increasing pain and swelling, prompting clindamycin treatment by the general practitioner. A subsequent CT-scan showed a submandibular collection with a superficial and deep component, accompanied by additional infiltration of the subcutaneous adipose tissue, focal skin thickening and lymph node enlargement (Figure 2).
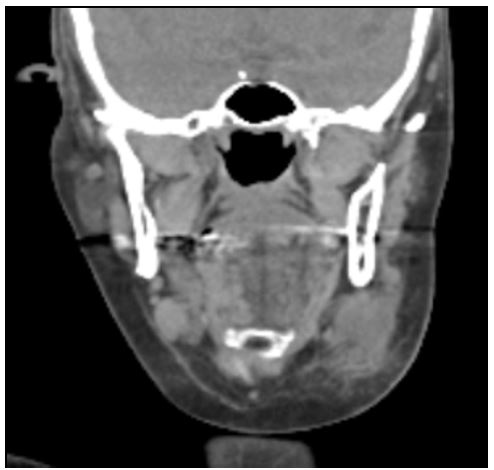
Figure 1: Coronal section of the initial CT-scan showing significant soft tissue swelling of the left submandibular region.
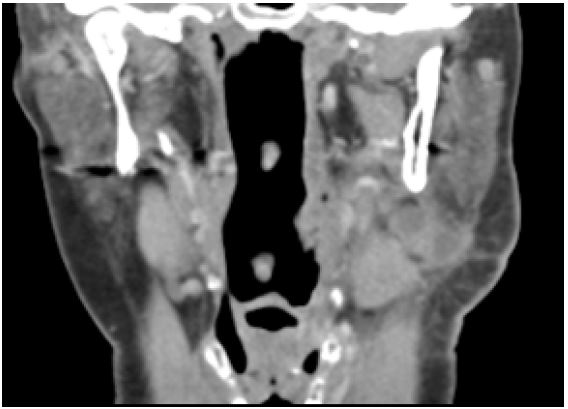
Figure 2: Coronal section of the CT-scan after the clinical stable period showing a left sided submandibular collection with a superficial and deep component, with infiltration of subcutaneous adipose tissue.
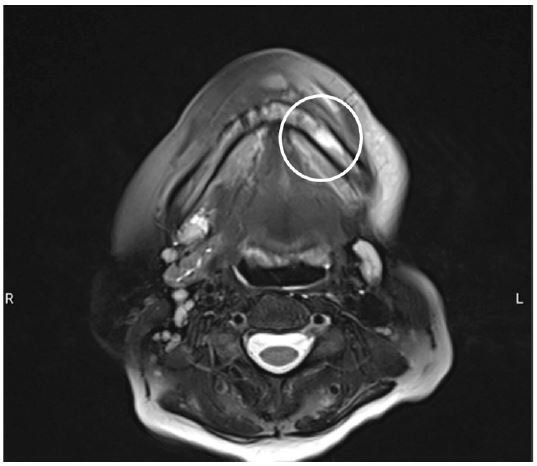
Figure 3: Transversal section on MRI, revealing a left sided increased signal intensity at the left mandibular corpus on T2-weighted images, consistent with mandibular osteomyelitis.
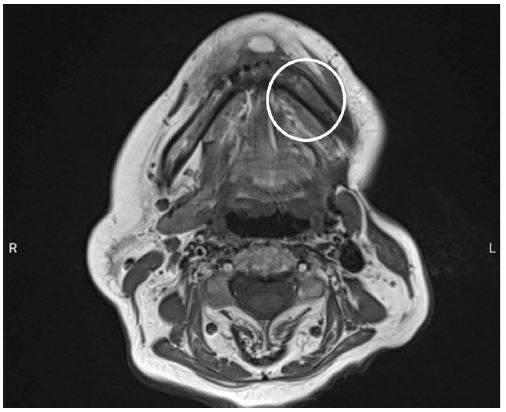
Figure 4: Transversal section on MRI, revealing a left sided decreased signal intensity at the left mandibular corpus on T1-weighted images, consistent with mandibular osteomyelitis.
The left submandibular salivary gland was removed due to the formation of an abscess. Histopathological examination confirmed supportive inflammation with an early granulomatous transformation. Subsequently, an episode of recurrent cervical collection necessitated a week-long admission to the Ear, Nose, Throat (ENT) department, where an Orthopantomograph (OPT) revealed tooth element 37, with no evidence of infection noted. Approximately four weeks post-admission, infliximab administration was interrupted again, due to another recurrence of the cervical abscess that mandated further drainage. Cultures revealed predominant white blood cells with minimal red blood cells. Streptococcus constellatus, sensitive to ampicillin, was once more identified, and the wound continued to produce pus. Two months later, the patient reported pain localized to the left mandibular region. A subsequent CT-scan showed soft tissue air inclusions, without noteworthy osteomyelitic changes or periosteal reactions. Notably, tooth element 37 was absent on this scan, having been previously extracted by the general dentist. Within nine days, the patient sought emergency care due to unbearable pain upon eating and drinking from a recurrent abscess, alongside long-standing numbness along the left mandible, anamnestically revealing incorrect occasional self-administration of amoxicillin/clavulanic acid as a means of pain relief. A Magnetic Resonance Imaging (MRI) scan confirmed left-sided osteomyelitis of the mandible, encouraging the patient’s referral to our department at the university hospital (Figures 3 and 4).
An admission was started, in which biopsies at the left mandibular corpus via bone probes were conducted, IV antibiotic was started, and a drain was placed. Cultures revealed Streptococcus mitis and Streptococcus parasanguinis. Initially, empirical IV treatment was started with 1 g/200 mg amoxicillin/clavulanic acid 6 dd. After completion of cultures, a transition to ceftriaxone 2 g 1dd IV was made. After a week, the drain was removed, and the patient was dismissed. A prolonged course of antibiotic therapy via Outpatient Parenteral Antibiotic Therapy (OPAT) was initiated for a total of 6 weeks. Based on the clinical progression under this therapy, the decision was made to extend this treatment to 12 weeks. Five weeks into this treatment, metronidazole 500 mg 3 dd IV was added. Further postoperative care included local mouth rinses, oral hygiene and pain management. Restarting infliximab is permissible once the infection is completely controlled.
The subsequent clinical developments indicated a reduction in swelling, persistence of the intra-oral pain and the fistula. The left-sided hypoesthesia has slightly improved but persists.
In the latest consultation, the intraoral pain had completely resolved, while the hypoesthesia persisted. The fistula had decreased in size and ceased to produce pus.
Discussion
This case reports documents the occurrence of mandibular osteomyelitis as a potential complication of a tooth extraction during infliximab treatment. The extraction of a mandibular molar acted as an entry point for oral pathogens and is in this case considered a precipitating factor in the development of osteomyelitis. Tooth extractions and oral surgery during infliximab treatment have previously been reported as risk factors for the development of osteomyelitis. A report by Ciantar et al. discussed the occurrence of mandibular osteomyelitis during infliximab treatment after the surgical extraction of the lower left third molar [3]. Another report by Tsuchiya et al. documented the occurrence of mandibular osteomyelitis after a pulpectomy during infliximab treatment [1].
The patient in this case report chronically suffered from cervical abscesses. Despite multiple drainage procedures, cultures and adequate antibiotic treatments, recurrences kept manifesting. When revising the history, a critical item was withheld when the patient reported that she occasionally took amoxicillin/clavulanic acid as form of pain relief, which raises the possibility that this may have contributed to resistance and recurrence of the causative micro-organisms.
Diagnostic challenges were encountered post-extraction, as the initial CT scan failed to detect mandibular osteomyelitis. The radiological diagnosis took place three months after the tooth extraction upon referral to our university hospital center. MRI, which is recognized for its sensitivity and specificity, eventually confirmed the diagnosis, and led to admission and bone probe sampling for appropriate treatment initiation [10].
Microbiological analysis identified Streptococcus mitis and Streptococcus parasanguinis as causative micro-organisms. There is however currently no consensus regarding the necessity of identifying the causative pathogen. Previous studies reported polymicrobial dentogenic micro-organisms as the cause of this infection. However, sample collection remains difficult in the oral cavity, given that samples are often contaminated by saliva which makes causative agents difficult to distinguish from contaminants [6,7]. Lucidarme et al. emphasized the identification of the causative pathogen as a priority in the diagnosis of chronical osteomyelitis of the jaw [11]. Other authors, for example André et al. stated that most of the germs in jaw osteomyelitis are sensitive to the association of amoxicillin/clavulanic acid or to clindamycin, making bacteriological investigations not of interest in the initial clinical management of these infections [6].
This was consistent with the management in both similar case reports, where no intra-operative sample collection was performed, and antibiotic treatment was started empirically. Despite the lack of intra-operative samples, the outcome in both cases after the antibiotic treatment was similar, and complete resolution occurred after 5 months [3] and 8 months [1] of follow-up time.
In addition to the clinical findings, the exact pathophysiological explanation of the development of osteomyelitis seems interesting. Infliximab is a chimeric human/mouse monoclonal antibody that exerts a suppressive effect on TNF-α, a critical immune mediator produced by macrophages and T-cells [12]. This suppression plays a role in the body’s immune response by regulating granuloma formation and intracellular pathogen elimination within macrophages, potentially increasing susceptibility to infections and disrupting bone turnover as well [13]. Infliximab’s mechanism of action involves binding to TNF-receptors, leading to cytokine suppression and apoptosis of producer cells, which may contribute to osteomyelitis development [3,13]. Furthermore, TNF-α’s negative impact on bone turnover, complicates the healing process post-extraction [14,15]. This was shown by Ferreira Junior et al, where the production of collagen type 1 in the tooth socket was limited in rats after a tooth extraction, resulting in less structural support and strength of the neoformed bone [15].
Despite their data suggesting that inhibition of TNF-α does not seem to alter bone repair under radiographic visualization, histological findings revealed less deposition of bone tissue and a greater amount of connective tissue in the group treated with infliximab.
Upon admission, in addition to bone probes, the patient in our case underwent abscess drainage and empirical treatment with amoxicillin/clavulanic acid infusions 1 g/200 mg 6 dd. Following culture results, the treatment shifted to ceftriaxone 2 g 1 dd, administered in OPAT setting. Multiple articles advocate for a minimum 6-week treatment duration [11,16,17]. Consistent with prior literature, anti-TNF- therapy is withheld until resolution of the infection occurs [18]. Additionally, the patient received instructions for local therapy involving mouth rinses with povidone-iodine mouthwash and maintaining optimal dental hygiene.
Considering the patient’s history, awareness should be present of the phenomenon of osteomyelitis and infliximab therapy. It is crucial to monitor treatment compliance in such patients, given that special consideration is needed for patients receiving infliximab therapy after dental extractions due to the increased risk of osteomyelitis. Considering this, prophylactic antibiotic may be beneficial for oral surgical interventions.
Acknowledgements: The authors did not receive support from any organization for the submitted work.
References
- Shuhei Tsuchiya KS, Masahiro Omori, Ryo Matsuda, Masahito Fujio, Hideharu Hibi. Mandibular osteomyelitis implicated in infliximab and periapical periodontitis: A case report. Journal of Oral and Maxillofacial Surgery, Medicine and Pathology. 2016: 410-5.
- Sacco R, Shah S, Leeson R, Moraschini V, de Almeida Barros Mourão CF, et al. Osteonecrosis and osteomyelitis of the jaw associated with tumour necrosis factor-alpha (TNF-α) inhibitors: A systematic review. Br J Oral Maxillofac Surg. 2020; 58(1): 25-33.
- Ciantar M, Adlam DM. Treatment with infliximab: Implications in oral surgery? A case report. Br J Oral Maxillofac Surg. 2007; 45(6): 507-10.
- Toussirot É, Bertolini E, Wendling D. Management of ankylosing spondylitis with infliximab. Open Access Rheumatol. 2009; 1: 69-82.
- Gerriets Valerie AG, Karam Khaddour. Tumor Necrosis Factor Inhibitors. In: Publishing S, editor.: Treasure Island. 2023.
- Andre CV, Khonsari RH, Ernenwein D, Goudot P, Ruhin B. Osteomyelitis of the jaws: A retrospective series of 40 patients. J Stomatol Oral Maxillofac Surg. 2017; 118(5): 261-4.
- Bertrand K, Lamy B, De Boutray M, Yachouh J, Galmiche S, et al. Osteomyelitis of the jaw: time to rethink the bone sampling strategy? Eur J Clin Microbiol Infect Dis. 2018; 37(6): 1071-80.
- Scolozzi P, Lombardi T, Edney T, Jaques B. Enteric bacteria mandibular osteomyelitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005; 99(6): e42-6.
- Lorè B, Gargari M, Ventucci E, Cagioli A, Nicolai G, et al. A complication following tooth extraction: chronic suppurative osteomyelitis. Oral Implantol (Rome). 2013; 6(2): 43-7.
- Pineda C, Espinosa R, Pena A. Radiographic imaging in osteomyelitis: The role of plain radiography, computed tomography, ultrasonography, magnetic resonance imaging, and scintigraphy. Semin Plast Surg. 2009; 23(2): 80-9.
- Lucidarme Q, Lebrun D, Vernet-Garnier V, Le Gall J, Diallo S, et al. Chronic Osteomyelitis of the Jaw: Pivotal Role of Microbiological Investigation and Multidisciplinary Management-A Case Report. Antibiotics (Basel). 2022; 11(5).
- Bruno Serolio SP, Alberto Sulli, Valentino Ferretti, Maurizio Cutolo. Bone Metabolism Changes During Anti-TNF-alpha therapy in Patients with Active Rheumatoid Arthritis. basic and clinical aspects of neuroendocrine immunology in rheumatic diseases. 2006; 1069(1): xiii-xxiv.
- Maksymowych WP, Jhangri GS, Lambert RG, Mallon C, Buenviaje H, et al. Infliximab in ankylosing spondylitis: A prospective observational inception cohort analysis of efficacy and safety. J Rheumatol. 2002; 29(5): 959-65.
- Haroon NN, Sriganthan J, Al Ghanim N, Inman RD, Cheung AM. Effect of TNF-alpha inhibitor treatment on bone mineral density in patients with ankylosing spondylitis: A systematic review and meta-analysis. Semin Arthritis Rheum. 2014; 44(2): 155-61.
- Ferreira-Junior AEC, Barros-Silva PG, Oliveira CC, Lima Verde MEQ, Sousa FB, et al. Influence of infliximab therapy on bone healing post-dental extraction in rats. Arch Oral Biol. 2020; 112: 104680.
- Lima AL, Oliveira PR, Carvalho VC, Cimerman S, Savio E. Recommendations for the treatment of osteomyelitis. Braz J Infect Dis. 2014; 18(5): 526-34.
- Spellberg B, Lipsky BA. Systemic antibiotic therapy for chronic osteomyelitis in adults. Clin Infect Dis. 2012; 54(3): 393-407.
- Strangfeld A, Listing J. Infection and musculoskeletal conditions: Bacterial and opportunistic infections during anti-TNF therapy. Best Pract Res Clin Rheumatol. 2006; 20(6): 1181-95.
