
Open Access, Volume 10
Autoimmune cytopenia that debuts with erythroleukemia
Roberto A Villa1 *; Giselle Begue2
1División Intensive Care, Hospital Juan A. Fernández, Buenos Aires, Argentina.
2Hematology, Hospital Juan A. Fernández, Buenos Aires, Argentina.
Dr. Arturo Giordano
Cardiovascular Interventions Unit, Pineta Grande Hospital, Domiziana Street KM 30, 81030 Castel Volturno CE, Italy
Phone/Fax: +39-336-945902
Email: arturogiordano@tin.it
Received : July 23, 2024,
Accepted : August 16, 2024
Published : August 30, 2024,
Archived : www.jclinmedcasereports.com
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Villa R (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Villa RA, Begue G. Autoimmune cytopenia that debuts with erythroleukemia. Open J Clin Med Case Rep. 2024; 2275.
Description
A 50-year-old woman suffering from lupus and antiphospholipid syndrome was admitted to the hospital for autoimmune anemia and thrombocytopenia. She received corticosteroid, immunoglobulin, and rituximab therapy. The patient presented with a drop in hematocrit and thrombocytopenia, as well as an elevated LDH level (>5000 IU/L) and shock, requiring mechanical ventilation and vasoactive support. In her peripheral blood smears (May-Giemsa, 100x), giant myeloid blasts with basophilic cytoplasm were observed (Figures 1A & 1B), which were not present in the previous 72 hours. Additionally, circulating erythroblasts were detected. The bone marrow biopsy showed a packed specimen, almost entirely composed of blasts (Figures 2C & 2D). Flow cytometry subsequently confirmed the diagnosis of erythroleukemia.
This case of Acute Erythroleukemia (AEL) is a rare and aggressive subtype of Acute Myeloid Leukemia (AML) characterized by erythroblastic proliferation. AEL accounts for less than 1% of all AML cases and has a very poor prognosis. According to the 2016 WHO definition of PEL, for the only type of acute leukemia with genuine erythroid differentiation, at least 80% of the marrow must consist of erythroid precursors, with at least 30% being proerythroblasts.
This case demonstrates the importance of conducting an acute peripheral blood morphological examination to guide treatment before definitive results are available.
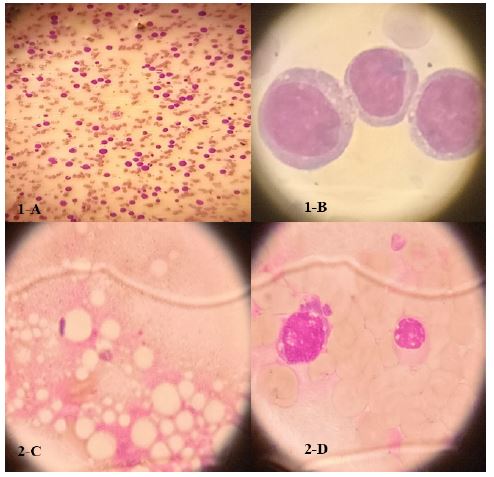
Figure 1 A-D: Clinical images.
