
Open Access, Volume 10
The impact of myoreflex therapy on patients with post-acute sequelae of covid-19
Baudrexl JC1; Schmidt Alba J1; Mosetter K2; Mosetter R2; Steinestel K3; Gagiannis D1
1Department of Pneumology, Bundeswehrkrankenhaus Ulm, 89081 Ulm, Oberer Eselsberg 40, Germany
2Center for Interdisciplinary Therapies, 78462 Konstanz, Obere Laube 44, Germany.
3Institute of Pathology and Molecular Pathology, Bundeswehrkrankenhaus Ulm, 89081 Ulm, Oberer Eselsberg 40, Germany.
Daniel Gagiannis
Department of Pneumology, Bundeswehrkrankenhaus Ulm, Oberer Eselsberg 40, 89081 Ulm, Germany.
Tel: 0049-731-1710-2901 & 0049-731-1710-2908;
Email: danielgagiannis@bundeswehr.org
Received : July 08, 2024,
Accepted : August 08, 2024
Published : August 15, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Background: There is an urgent need for new therapeutic options concerning patients with Post-Acute Sequelae of COVID-19 (PASC). Non-specific complaints such as cognitive impairment, reduced physical ability, shortness of breath, fatigue syndrome, arthritic and musculoskeletal pain restrain the overall quality of life.
Objectives: This is a randomized, placebo-controlled, single-blind study. The period of observation went from July 2020 to August 2023. 142 patients were enrolled in the study. All patients gave written informed consent. Myoreflex therapy was performed on patients with PASC in order to enhance physical performance and improve the overall wellbeing of the patients.
Methods: 67 of the 142 patients each received 5 sessions of myoreflex therapy. The influence of myoreflex therapy on patients was assessed through testing of the pulmonary function. Continuous variables were tested between groups using Wilcoxon rank sum test. Categorial variables were tested using Pearson’s Chi-squared tests. In addition, a multiple group comparison (ANOVA/Tukey) was carried out to verify the results.
Results: Patients who received myoreflex therapy showed a significant improvement in diffusion capacity and diffusion performance compared to patients who did not receive myoreflex therapy.
Conclusion: Previous studies have shown a significant improvement in diffusion capacity after 6 weeks of intensive pulmonary rehabilitation. We are the first research group to demonstrate a similar effect after 5 sessions of myoreflex therapy. According to our results, myoreflex therapy seems to have a positive effect on lung function, especially on diffusion capacity. Overall, this supports the theory that the musculature appears to play a central role in the generalized inflammatory processes associated with PASC.
Keywords: COVID-19; SARS-CoV-2; PASC; Long COVID; Post COVID; Myoreflex therapy.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Gagiannis D (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Baudrexl JC, Alba JS, Mosetter K, Mosetter R, Steinestel K, Gagiannis D. The impact of myoreflex therapy on patients with post-acute sequelae of covid-19. Open J Clin Med Case Rep. 2024; 2272.
Introduction
In December 2019 one of the greatest pandemics of our time started with the first COVID-19 cases reported in Wuhan, China [1]. Over 771.407.825 people were infected with the SARS-CoV-2 Virus and over 6.972.152 deaths were reported according to the World Health Organization [2]. In Comparison the Influenza pandemic in 1918 also known as the “Spanish flu” caused over 500 million infected people and nearly 50 million deaths worldwide [3,4]. The echo of the COVID-19 pandemic is still perceptible in our society. Approximately 10-30% of the people infected with the SARS-CoV-2-Virus developed ongoing symptoms within 3 months after confirmed infection that last over 2 months [5] and are labeled as Post-Acute Sequelae of COVID-19 (PASC). This aspect does not only affect the healthcare systems worldwide but also compromises global economy. Nearly one-third of the patients with Post-Acute Sequelae of COVID-19 (PASC) is in need of a reduced work schedule compared to the healthier state prior to the infection. Additionally due to persistent symptoms one-third of the patients is not able to return to full workforce at 7 months of follow up [6]. These persisting symptoms are mainly non-specific and heterogeneous. Research has shown over hundreds of complaints related to SARS-CoV-2 infection. The most frequently described manifestations of Post-acute sequelae of COVID-19 are cognitive impairment, reduced physical ability, shortness of breath, fatigue syndrome, arthritic and musculoskeletal pain [7]. Presumably the restriction in daily activities such as running the household or the reduced physical performance restrain one´s quality of life. Until now there is no concrete therapy regime that can be offered to patients with non-specific symptoms of PASC. There is urgent need to improve physical performance and quality of life.
In order to enhance physical performance Myoreflex therapy is frequently used in high-performance sports [8-10]. Myoreflex therapy is a holistic therapy concept combining the most effective therapeutic aspects of Chinese medicine, acupuncture, physiotherapy, manual therapy, orthopedics and biomechanics [11,12]. By improving the interaction of the musculoskeletal structures an overall improvement in mobility and the optimization of the movement can be achieved, thus making the course of movement become physiological [9-11]. In order to analyze pain and its source the therapist examines the relevant “kinetic chains”. A kinetic chain consists of all structures of the musculoskeletal system involved and interacting in a particular movement. There is a constant interaction of agonists and antagonists resulting in a particular movement such as walking, running etc. In order to generate an economical movement sequence the interaction of agonists and antagonists, contiguous joints and soft tissue structures needs to be accurately coordinated. Muscular imbalance, increased muscular tension and the resulting incorrect stress load on joints, can lead to the development of pain, postural anomalies and, in the long term, arthrosis. In order to analyze the source of pain, the therapist identifies the responsible kinetic chains [12]. Increased basic tension in the muscle of the patient is identified through structured palpation. By applying manual pressure, the therapist stimulates these areas of increased muscular tension until a noticeable relaxation takes place. The change in basic tension, and thus muscular dysregulation, is reported to the central nervous system via Golgi tendon receptors, muscle spindles, and adjoined afferences. Through this feedback mechanism, muscular imbalances and misalignments are reported and counter-regulation can occur. Muscle-tendon junctions are often the target of pressure point stimulation, as the underlying increased muscle tone can often be detected here. These points coincide with target points of acupuncture and neural therapy [12].
Based on existing data, it is assumed that Myoreflex therapy can reduce non-specific PASC symptoms and improve subjective dyspnea and lung function. Myoreflex therapy has already shown to significantly improve mobility and to reduce pain by releasing basic tension in muscles and correct misalignments and unphysiological stress load on joints and soft tissue structures. Therefore, Myoreflex therapy has been included in the exercise routine of the US national Soccer Team and other high-performance sports [8-10]. This is the first study analyzing the effects of Myoreflex therapy on the pulmonary function of patients with PASC and non-specific symptoms.
Methods
This study was conducted as a randomized, placebo-controlled, single-blind study at the German Military Hospital in Ulm, Germany. Participants were randomized by lot from third parties not involved in the study and received Myoreflex therapy or traditional physiotherapy consisting of respiratory therapy and manual therapy for the duration of the entire intervention period. Patients were informed that they would receive either a new or an established form of physiotherapy if they participated in the study. Further details were omitted to ensure single blinding and thus better objectification of the results. The basic drug therapy of PASC corresponded to the standard of care and was the same in both groups. The decoding of group membership took place after the intervention phase following evaluation of the lung function tests. The period of observation went from July 2020 to August 2023. 142 patients were enrolled in the study. All patients gave written informed consent. Patients included in the study had a positive PCR test for SARS-CoV-2 previously and ongoing non-specific PASC symptoms over 3 months such as fatigue-syndrome, cognitive impairment, reduced physical performance, dyspnea related to exertion etc. An extensive anamnesis, radiographic examination, detailed laboratory examination, bronchoscopy with biopsy of lung tissue, pulmonary function diagnostics and guideline-based drug therapy was performed on the patients. Subsequently, patients with persistent non-specific symptoms received either five sessions of myoreflex therapy (n=67) or conventional physiotherapy (n=75) after prior simple, unrestricted randomization. The study was approved by the ethics committee of the University of Ulm. Demonstration of data was based on the suggestions of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) initiative. This research was performed in conformity with the ethical standards of the institutional research committee. For this non-interventional observational prospective study, the collected data were anonymized and all Patients gave written informed consent. Safeguarding of data was strictly assured.
Statistical analysis: Continuous variables were tested between groups using Wilcoxon rank sum test. Categorial variables were tested using Pearson’s Chi-squared tests. P-values were adjusted for multiple testing using a Bonferroni correction. Level of significance was set to alpha = 0.05.
In addition, a multiple group comparison (ANOVA/Tukey) was carried out to verify the results.
Results
A total of 142 patients were recruited for this study. 67 patients received five sessions of myoreflex therapy and 75 patients received five sessions of traditional physiotherapy consisting of breathing therapy and manual therapy. All patients experienced mild COVID-19 without the need for hospitalization in the acute phase. The diagnosis of COVID-19 was on average 20 weeks ago. The average age of the study participants was 40 years. In addition, none of the patients had a relevant previous illness. The lung function parameters recorded before and after the respective therapy series are shown in Tables 1 to 3. The present analysis showed that Diffusion Capacity (DLCO and KCO) improved significantly (p< 0.001) in patients after myoreflex therapy compared to patients who received conventional treatment (Table 3; Figures 1 & 2). The other parameters of lung function also showed a positive trend (Table 3). The additional ANOVA/Tukey analysis showed comparable results. DLCO and KCO after myoreflex therapy showed a significant improvement (p< 0.05) for both parameters.
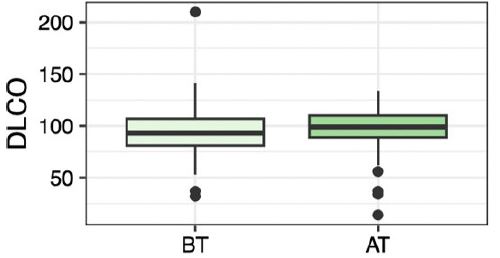
Figure 1: Comparing DLCO before (BT) and after (AT) Myoreflex therapy. It shows a highly significant improvement in DLCO in patients who received myoreflex therapy.
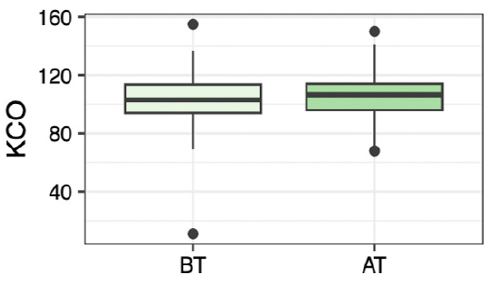
Figure 2: Comparing KCO before (BT) and after (AT) Myoreflex therapy. There ist a highly significant improvement in KCO in patients who received myoreflex therapy.
Table 1: Descriptive data and parameters of pulmonary function before Myoreflex therapy.
| Characteristics | Overall, N=142 | No-Myoreflex therapy N=75 | Myoreflex therapy N=67 | p-value1 |
|---|---|---|---|---|
| ID, median(IQR) | 72(36, 126) | 61(31, 132) | 77(45, 123) | 0.402 |
| Sex, n(%) | 0.098 | |||
| male | 74(52%) | 44(59%) | 30(45%) | |
| female | 68(48%) | 31(41%) | 37(55%) | |
| Age, median(IQR) | 40(28, 54) | 40(28, 55) | 38(28, 52) | 0.592 |
| Weeks sinceCovid, median (IQR) | 20(14, 38) | 20(12, 38) | 22(16, 36) | 0.318 |
| Spirometry | ||||
| FVC, median(IQR) | 93(82, 104) | 93(86, 103) | 92(86, 103) | 0.902 |
| FEV1, median(IQR) | 93(82, 104) | 94(83, 105) | 91(82, 101) | 0.438 |
| FEV1/FVC, median (IQR) | 90(81, 100) | 90(81, 100) | 91(80, 100) | 0.939 |
| MEF50, median(IQR) | 87(68, 100) | 91(72, 109) | 85(63, 97) | 0.033 |
| Lung volume | ||||
| TLC, median(IQR) | 102(92, 115) | 102(91, 112) | 102(95,116) | 0.287 |
| RV/TLC, median(IQR) | 109(90, 122) | 103(90, 118) | 111(93, 129) | 0.256 |
| Diffusion capacity | ||||
| DLCO, median(IQR) | 93(81, 107) | 94(84, 108) | 92(81, 105) | 0.549 |
| KCO, median (IQR) | 102(93, 113) | 107(94, 117) | 99(93, 109) | 0.025 |
Data are presented as n, median (IQR=Interquartile Range), n (%) and parameters of pulmonary function were given in percent. 1Wilcoxon rank sum test. Variables were tested using Pearson’s Chi-squared tests. Weeks since Covid: Weeks since first diagnosis of COVID-19; FVC: Forced Vital Capacity; FEV1: Forced Expiratory Volume in 1 s; MEF50: Mean Expiratory Flow at 50% of FVC; TLC: Total Lung Capacity; RV: Residual Volume; DLCO: Diffusing Capacity of the Lung for Carbon Monoxide; KCO: factor for carbon monoxide absorption of the lung.
Table 2: Parameters of pulmonary function after Myoreflex therapy.
| Characteristics | Overall, N=142 | No-Myoreflex therapy N=75 | Myoreflex therapy N=67 | p-value1 |
|---|---|---|---|---|
| Spirometry | ||||
| FVC, median (IQR) | 95(88, 105) | 96(88, 105) | 94(87, 105) | 0.706 |
| FEV1, median (IQR) | 96(86, 106) | 96(88, 109) | 94(83, 104) | 0.243 |
| FEV1/FVC, median (IQR) | 82(77, 87) | 81(78, 86) | 82(77, 87) | 0.947 |
| MEF50, median (IQR) | 88(74, 103) | 94(78, 113) | 85(68, 96) | 0.024 |
| Lung volume | ||||
| TLC, median (IQR) | 106(93, 115) | 103(91, 113) | 107(99, 117) | 0.182 |
| RV/TLC, median (IQR) | 103(89, 121) | 101(84, 119) | 106(92, 124) | 0.158 |
| Diffusion capacity | ||||
| DLCO, median (IQR) | 100(89, 111) | 97(83, 104) | 102(92, 114) | 0.015 |
| KCO, median (IQR) | 108(95, 115) | 102(92, 112) | 109(103, 118) | 0.002 |
Data are presented as n, median (IQR=Interquartile Range), n (%) and parameters of pulmonary function were given in percent.1 Wilcoxon rank sum test. Variables were tested using Pearson’s Chi-squared tests. Weeks since Covid: Weeks since first diagnosis of COVID-19; FVC: forced vital capacity; FEV1: Forced Expiratory Volume in 1 s; MEF50: Mean Expiratory Flow at 50% of FVC; TLC: Total Lung Capacity; RV: Residual Volume; DLCO: Diffusing Capacity of the Lung for Carbon Monoxide; KCO: factor for carbon monoxide absorption of the lung.
Table 3: Differences in parameters of pulmonary function after minus before Myoreflex therapy.
| Characteristics | Overall, N=142 | No-Myoreflex therapy N=75 | Myoreflex therapy N=67 | p-value1 |
|---|---|---|---|---|
| Spirometry | ||||
| FVC, median (IQR) | 1(-3,5) | -1(-4,5) | 1(-3,6) | 0.242 |
| FEV1, median(IQR) | 1(-4,7) | 0(-4,7) | 1(-4,7) | 0.616 |
| FEV1/FVC, median (IQR) | -4(-16,1) | -3(-15,1) | -5(-19,1) | 0.506 |
| MEF50, median(IQR) | 0(-8,8) | 0(-7,8) | 0(-8,8) | 0.751 |
| Lung volume | ||||
| TLC, median(IQR) | 1(-6,8) | 0(-6,7) | 1(-7,11) | 0.730 |
| RV/TLC, median(IQR) | -4(-21,13) | -4(-17,16) | -3(-27,12) | 0.403 |
| Diffusion capacity | ||||
| DLCO, median(IQR) | 2(-4,10) | 0(-10,2) | 6(0,18) | <0.001 |
| KCO, median (IQR) | 3(-4,10) | -3(-10,0) | 8(3,16) | <0.001 |
Data are presented as n, median (IQR=Interquartile Range), n (%) and parameters of pulmonary function were given in percent.1 Wilcoxon rank sum test. Variables were tested using Pearson’s Chi-squared tests. Weeks since Covid: Weeks since first diagnosis of COVID-19; FVC: Forced Vital Capacity; FEV1: Forced Expiratory Volume in 1 s; MEF50: Mean Expiratory Flow at 50% of FVC; TLC: Total Lung Capacity; RV: residual volume; DLCO: Diffusing Capacity of the Lung for Carbon Monoxide; KCO: factor for carbon monoxide absorption of the lung.
Discussion
In this study, myoreflex therapy is described as a non-pharmacological procedure that can achieve significant improvements in lung function parameters, in particular diffusion capacity, in patients with PASC after only a short period of time. Previous studies have shown that COVID-19 can be associated with a higher degree of damage to alveolar cells and lung structure [13]. The pathological changes can be caused directly by the viral infection or secondarily by an excessive inflammatory response [14]. This leads to diffuse alveolar damage [15]. 30% of patients who survive severe COVID-19 develop persistent impairment of lung function. 10% of those affected also develop radiologically and histologically detectable airway pathology such as fibrotic lung damage [16]. Almost one third of patients with PASC and persistent dyspnea were found to have a reduced diffusion capacity [17,18]. Restrictive pulmonary changes and an associated reduced diffusion capacity after acute lung diseases have been shown to contribute to long-term functional impairment and lead to a reduced health-related quality of life [19,20]. A reduced diffusion capacity was also detected in the present study in patients with previously mild COVID-19. Damage to the interface between the alveolus and capillaries is discussed in the literature as a possible correlate. This theory was supported by an exploratory hyperpolarized 129Xe MRI analysis [20]. It is not yet clear whether patients with PASC and reduced diffusion capacity develop pulmonary fibrosis. As these are very slow processes, we will have to wait and see over the next few years. However, in a Chinese study 20% of PASC patients showed a persistently reduced diffusion capacity. In this case, the accompanying CT scan showed the onset of pulmonary fibrosis, which supports the importance of DLCO measurement and early improvement [22]. Several studies have already shown that there was a significant improvement in lung function after 6 weeks of pulmonary rehabilitation in patients with PASC [23,24]. In the present analysis, a significant improvement was also observed, albeit after only five outpatient sessions of Myoreflex therapy. The rehabilitation success was attributed by Liu et al. [23] to the strengthening of the auxiliary respiratory muscles. The significant improvement in diffusion capacity in patients receiving Myoreflex therapy suggests that the inflammatory process in the lung parenchyma and the suspected alveolar damage might be positively influenced by Myoreflex therapy. The underlying pathomechanism still needs to be investigated in more detail. Several limiting aspects must be taken into account when interpreting the results of our study. Due to the fact that the pathomechanisms of PASC have not yet been fully elucidated and due to the basic design of the study, it is not possible to provide clear evidence of a correlation between myoreflex therapy and the improvement in lung function. The comparison group only received conventional physiotherapy and no myoreflex therapy with therapeutically ineffective points. A true placebo control as a comparison arm could therefore not be guaranteed. The observed improvements in lung function could in principle also be due to the normal healing process of the lungs or greater attention to the patient. Nevertheless, the assumption that Myoreflex therapy has a positive influence on the improvement of lung function can be justified by the significantly higher benefits in patients who received therapy. The results of this study cannot be applied to the entire population of PASC patients, as the present study population was younger and had fewer pre-existing diseases than in comparable studies. However, this in turn is also a strength of the study, as such a clientele has not been investigated in any previous work. Due to the positive aspects of Myoreflex therapy already established in high-performance sports and the indications of a positive influence on lung function presented in this analysis, subsequent studies should also look at further possible effects of Myoreflex therapy on other non-specific symptoms in PASC. Especially a possible improvement in fatigue-syndrome or cognitive impairments should be investigated.
Conclusion
Myoreflex therapy offers a time-saving alternative to current lengthy rehabilitation process and has been shown to lead to at least an equivalent improvement in lung function. It was shown that patients who received Myoreflex therapy had a significant improvement in diffusion capacity. The investigation of further possible positive effects of Myoreflex therapy in PASC patients with non-specific symptoms should be considered in following studies.
Highlights
- In top-level sport, PACS has repeatedly put an end to careers. For the first time, myoreflex therapy shows a significant improvement in the diffusion performance of the lungs by treating the muscles. This illustrates the connection between previously unspecific myopathy and a resulting generalized inflammatory reaction.
- PASC also means that many amateur athletes are no longer able to reproduce the training goals they previously achieved without any problems. In some cases, they even have to give up sport completely. Myoreflex therapy can restore the ability to train.
- This study illustrates the need for a multidisciplinary concept and not just the treatment of one organ, such as the lungs themselves.
- We were also able to show that missing baseline values of previously presumed healthy individuals suggest falsely normal lung function values. By comparison in the field of sports, where individual baseline values were available before COVID-19, even a KCO value of 100% can therefore be significantly lower (if it was previously 140%, for example) and thus clinically significant.
- Myoreflex therapy offers a time-saving alternative compared to current long lasting rehabilitation and has shown evidence of equivalent improvement in lung function. It was shown that patients who received Myoreflex therapy had a significant improvement in diffusion capacity.
Declarations
Acknowledgements: The authors would like to thank all patients for their consent to the use of data and images in the present study.
Funding: None.
Declaration of interest: DG was speaker for Boehringer-Ingelheim, MSD, Berlin Chemie, Pfizer and AstraZeneca. KS was speaker for Boehringer-Ingelheim. All other authors declare no conflict of interest.
Author contributions: Study concept: JB and DG. Data collection: JB, JS, DG, KS. Sample collection: JB, DG, KS. Initial draft of manuscript: DG. Critical revision and approval of final version: all authors.
Confirmation of ethical compliance: The study was approved by the ethics committee of the University of Ulm (reference no. 129-20) and was conducted in accordance with the Declaration of Helsinki.
Key messages
Myoreflex therapy is an outstanding and unique therapy concept that provides long-term benefits for the patients. This work explains for the first time on a scientific level the basic principles and underpins them with a summary of pre-described individual cases. Myoreflex therapy is a suitable procedure for complementary use in cases of long-lasting performance deficits such as Post-Acute COVID Syndrome (PACS). Treatment of the musculature has a significant influence on the normalization of lung function parameters, which is indicative of generalized inflammation involving the musculature in PACS patients.
References
- David J. Sencer. COVID-19 Timeline. COVID-19 Timeline. 2023. Verfügbar unter: https://www.cdc.gov/museum/timeline/covid19.html
- World Health Organisation. WHO Coronavirus (Covid-19) Dashboard [Internet]. WHO Coronavirus (COVID-19) Dashboard. 2023. Verfügbar unter: https://covid19.who.int
- Liang ST, Liang LT, Rosen JM. COVID-19: A comparison to the 1918 influenza and how we can defeat it. Postgrad Med J. 2021; 97(1147): 273-4.
- Barry JM. The great influenza: The story of the deadliest pandemic in history. New York: Penguin Books. 2021.
- Parotto M, Gyöngyösi M, Howe K, Myatra SN, Ranzani O, et al. Post-acute sequelae of COVID-19: understanding and addressing the burden of multisystem manifestations. Lancet Respir Med. 2023; 11(8): 739-54.
- Nalbandian A, Sehgal K, Gupta A, Madhavan MV, Mc Groder C, et al. Post-acute COVID-19 syndrome. Nat Med. 2021; 27(4): 601-15.
- Aiyegbusi OL, Hughes SE, Turner G, Rivera SC, McMullan C, et al. Symptoms, complications and management of long COVID: A review. J R Soc Med. 2021; 114(9): 428-42.
- Mosetter K. Myoreflexkonzept Schmerzfrei über die Physik funktioneller Anatomie. Med Sports Netw. 2012; 1(7): 1-58.
- Mosetter K. Myoreflextherapie im Sport: Fälle aus der Praxis. Erfahrungsheilkunde. 2018; 67(03): 169-73.
- Mosetter K. Schmerzen erfolgreich behandeln mit Myoreflextherapie. Erfahrungsheilkunde. 2018; 67(03): 160-8.
- Bick P. Myoreflextherapie-ein Konzept mit breitem Wirkungsspektrum. Myoreflextherapie-ein Konzept mit breitem Wirkungsspektrum. 2023. Verfügbar unter: https://osteopathie-bick.de/wp-71ff7-content/uploads/2020/02/Praxis_ergotherapie.pdf
- Mosetter K, Mosetter R. Myoreflextherapie / Kurt Mosetter. Bd. 1: Einführung in Muskelfunktion und Schmerz. 2., korr. Aufl. Konstanz: Vesalius-Verl. 2006; 242.
- Shao H, Qin Z, Geng B, Wu J, Zhang L, et al. Impaired lung regeneration after SARS‐CoV‐2 infection. Cell Prolif. 2020; 53(12): e12927.
- Schurink B, Roos E, Radonic T, Barbe E, Bouman CSC, et al. Viral presence and immunopathology in patients with lethal COVID-19: A prospective autopsy cohort study. Lancet Microbe. 2020; 1(7): e290-9.
- Peiris S, Mesa H, Aysola A, Manivel J, Toledo J, et al. Pathological findings in organs and tissues of patients with COVID-19: A systematic review. Ten Cate H, Herausgeber. PLOS ONE. 2021; 16(4): e0250708.
- Bazdyrev E, Rusina P, Panova M, Novikov F, Grishagin I, et al. Lung Fibrosis after COVID-19: Treatment Prospects. Pharmaceuticals. 2021; 14(8): 807.
- Tanni SE, Fabro AT, De Albuquerque A, Ferreira EVM, Verrastro CGY, et al. Pulmonary fibrosis secondary to COVID-19: a narrative review. Expert Rev Respir Med. 2021; 15(6): 791-803.
- Singh SJ, Baldwin MM, Daynes E, Evans RA, Greening NJ, Jenkins RG, u. a. Respiratory sequelae of COVID-19: pulmonary and extrapulmonary origins, and approaches to clinical care and rehabilitation. Lancet Respir Med. 2023; 11(8): 709-25.
- Burnham EL, Hyzy RC, Paine R, Coley C, Kelly AM, et al. Chest CT Features are Associated With Poorer Quality of Life in Acute Lung Injury Survivors: Crit Care Med. 2013; 41(2): 445-56.
- Grist JT, Collier GJ, Walters H, Kim M, Chen M, et al. Lung Abnormalities Detected with Hyperpolarized 129 Xe MRI in Patients with Long COVID. Radiology. 2022; 305(3): 709-17.
- Marvisi M, Ferrozzi F, Balzarini L, Mancini C, Ramponi S, et al. First report on clinical and radiological features of COVID-19 pneumonitis in a Caucasian population: Factors predicting fibrotic evolution. Int J Infect Dis. Oktober 2020; 99: 485-8.
- Liang L, Yang B, Jiang N, Fu W, He X, et al. Three-Month Follow-Up Study of Survivors of Coronavirus Disease 2019 after Discharge. J Korean Med Sci. 2020; 35(47): e418.
- Liu K, Zhang W, Yang Y, Zhang J, Li Y, Chen Y. Respiratory rehabilitation in elderly patients with COVID-19: A randomized controlled study. Complement Ther Clin Pract. Mai 2020; 39: 101166.
- Nopp S, Moik F, Klok FA, Gattinger D, Petrovic M, et al. Outpatient Pulmonary Rehabilitation in Patients with Long COVID Improves Exercise Capacity, Functional Status, Dyspnea, Fatigue, and Quality of Life. Respiration. 2022; 101(6): 593-601.
