
Open Access, Volume 10
Clinical and epidemiological features of manifestations of hapillomavirus infection in Baku
Sh Q Kadimova*
Azerbaijan Medical University, Baku, Azerbaijan.
Sh Q Kadimova
Azerbaijan Medical University, Baku, Azerbaijan.
Email: shayman848gmail.ru
Received : July 07, 2024,
Accepted : August 05, 2024
Published : August 15, 2024,
Archived : www.jclinmedcasereports.com
Abstract
The conducted studies examined the clinical and epidemiological features of the manifestations of human papillomavirus infection in Baku. To achieve the purpose of the study, based on developed clinical and laboratory criteria, for the period from 2021 to 2023. 96 women aged 18-65 years (mean age 41.5 years) were recruited and underwent cervical cytology and human papillomavirus testing. Two groups were formed: the main group - 64 women with identified High-Risk Human Papillomavirus (HPV-HR) (16, 18, 36, 45 genotypes), the control group - 32 women with a negative result of HPV testing. Due to the widespread spread of the human papillomavirus in recent years, its socio-economic significance and the insufficient volume of preventive measures taken for this disease, an increase in the level of infection of women with this infection has been observed. The data obtained during the study show the polysystemic nature of the identified disorders that occur during infection with human papillomavirus infection and indicate the presence in patients with subclinical forms of human papillomavirus infection of medical and social factors that create an unfavorable premorbid background and cause the transition of the infection from the subclinical form to the clinical one.
Keywords: Papillomavirus infection; Human papilloma virus; Cervical cancer; Prevention; Vaccination; Quadrivalent vaccine; Girls; Adolescents.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Kadimova SQ (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Kadimova SQ. Clinical and epidemiological features of manifestations of hapillomavirus infection in Baku. Open J Clin Med Case Rep. 2024; 2271.
Introduction
Human Papillomavirus Infection (HPV) is the leading cause of invasive squamous cell carcinoma of the cervix and cancer mortality among women of reproductive age worldwide [1-3]. Therefore, prevention of cervical cancer depends primarily on preventing infection through vaccination against human papillomavirus (primary prevention) and identifying and treating precancerous lesions (also known as high-grade cervical intraepithelial neoplasia (CIN2/3) or Adenocarcinoma In Situ (ACIS)) before they develop into cancer (secondary prevention) [4]. Cervical cancer is the fourth most common cancer among women worldwide, with a global incidence of 13.3 per 100,000 women in 2020 [5]. Population-based and randomized studies show that vaccination against Human Papillomavirus (HPV) reduces the incidence of cervical precancerous diseases [6,7]. These data indicate that the vaccine reduces the incidence of cervical cancer, but vaccination coverage against human papillomavirus is insufficient in many countries, including Azerbaijan.
In its Global Strategy to Accelerate the Elimination of Cervical Cancer as a Public Health Problem, WHO has set a goal for 194 countries to adopt human papillomavirus vaccination by 2030. As of December 2021, all European Union/European Economic Area countries have included human papillomavirus vaccination in their national vaccination schedules. All recommendations call for two doses of HPV vaccination for girls aged 9-14 years, although the starting age varies by country. If vaccination begins after age 15 or if the person is immunocompromised, most recommendations call for three doses of the vaccine. In April 2022, the WHO Strategic Advisory Group of Experts on Immunization updated its recommendations on human papillomavirus vaccine dosage as follows: one or two doses for the primary target group of girls aged 9-14 years; one or two doses for young women aged 15-20 years; two doses six months apart for women over 21 years of age.
Since 2019, the human papillomavirus vaccine has been administered at the National Cancer Center of Azerbaijan. However, since the HPV vaccine is not included in the national vaccination schedule in the republic, it is paid for. In Azerbaijan, all boys and girls aged 11-12 years are recommended to be vaccinated. If the vaccination was not carried out in this age period, vaccination is recommended until the age of 21 for boys and until the age of 26 for girls. In the future, it is planned to include the HPV vaccine in the national vaccination schedule. Complete elimination of cervical cancer can be achieved through increased use of human papillomavirus vaccination and efforts to expand cervical cancer screening [8,9].
The purpose of this study was to study the clinical and epidemiological features of the manifestations of human papillomavirus infection in Baku.
Material and Methods
In our work, to achieve the goal of the study, based on developed clinical and laboratory criteria, for the period from 2021 to 2023. 96 women aged 18-65 years (average age 41.5 years) were selected who underwent cervical cytology and HPV testing at the Department of Obstetrics and Gynecology II of the AMU and the Training and Surgical Center of the AMU. Two groups were formed: the main group - 64 women with identified High-Risk Human Papillomavirus (HPV-HR) (16, 18, 36, 45 genotypes), the control group - 32 women with a negative result of HPV testing. The groups were formed according to the principle of continuous selection using random and typological sampling - using the method of balanced groups identical in age, social, educational and family status. The criteria for inclusion in the groups were: the presence of a preliminary diagnosis of inflammatory disease of the cervix, the presence of an HPV oncotype (or its absence), the absence of changes in the cervix as a consequence of the birth process or diagnostic procedures, had not recently taken vaginal medications/irrigations, the age of the subjects was from 18 to 65 years old. The criteria for exclusion from the groups were: women’s age over 65 years and under 18 years, cervical neoplasm, hypertrophy and glandular cyst; postpartum changes in the cervix, traumatic injuries to the cervix during diagnostic or therapeutic procedures, specific infections and sexually transmitted infections.
Vaccination was carried out with the Gardasil-4 vaccine, which protects against four types of papillomavirus: 16, 18, and 6, 11, which cause genital warts. Vaccination of girls and women is carried out between the ages of 9 and 45 years, and boys and men from 9 to 26 years. The examination of women, in addition to the mandatory study of obstetric-gynecological and somatic history, included the collection of data on hereditary history (in particular, cancer), menarche, the nature of specific functions (menstrual and secretory), characteristics of sexual life (time of its onset, number of partners, methods of contraception). Patients provided information about their place of work and contact with occupational hazards. The obtained data on the health status and medical history of women was entered into a specially designed questionnaire to simplify the statistical processing of the results. An objective examination of women (in addition to general clinical parameters) included mandatory extended colposcopy with photographic recording of the results. Next, a preliminary diagnosis was made, additional examinations were prescribed, and patient management tactics were determined.
Colposcopy was performed using the KS-02 optical system (model 51), recording was carried out with a Nokia digital camera (resolution 96 pixels per inch). Before the study, a smear was taken from each woman to determine the degree of purity of the vaginal contents, a bacteriological examination of the contents of the cervical canal was carried out to determine sensitivity to antibacterial drugs, a PCR study was carried out for the presence of sexually transmitted infections, such as mycoplasma, ureaplasma, chlamydia and determined strain of human papillomavirus. When an inflammatory reaction was detected, sanitation of the genital tract was carried out, anti-inflammatory treatment, if necessary, taking into account the presence of pathogenic flora, after which extended colposcopy was performed.
Diagnostics by polymerase chain reaction was carried out using a Rotor Gene 6000 amplifier. To carry out the analysis, the contents of the cervical canal were taken with a urogenital probe into an Eppendorf tube containing a preservative solution. The collected samples were delivered to the laboratory within 2 hours. The following types of HPV were determined using the polymerase chain reaction method: 6, 11, 16, 18, 31, 33, 35, 39, 42, 43, 44, 45, 52, 54, 56, 58, 59, 66.
Statistical analysis
Baseline characteristics are summarized as proportions and mean ± standard deviation. The sample parameters given in the tables have the following designations: M- mean, σ- standard deviation, n-volume of the analyzed subgroup, p-achieved level of significance. In the case of a normal distribution, a statistically significant difference in sample means was tested using Student’s t test; in other cases, the nonparametric Mann-Whitney test was used. Testing for statistical significance of differences between the relative frequencies of two or more events was carried out using the χ2 test.
Results and Discussion
Considering the fact that HPV strains of high oncogenic risk are important in the process of malignancy, we included in the main group women carriers of HPV types 16, 18, 36 and 45. Note that a single strain was not identified in any patient. A predominantly combination of 16, 18 and 36 strains was observed - in 44 patients (68.8±5.7%), in 8 (12.5±4.2%) a combination of 18 and 36 strains was recorded, and in the remaining 12 (18.7±4.9%) – a combination of 36 and 45 types. Since all isolated strains of the HPV virus belong to a group of high cancer risk, we did not further distribute the women into subgroups, and interpreted the results obtained in relation to the entire main group. To assess risk factors, a retrospective case-control study was conducted among 96 examined women aged 18-65 years. Risk factors were assessed based on survey data. The distribution by age groups is presented in Table1.
Table 1: Age groups among women with positive and negative HPV test results.
| Age groups,years | Main group (n=64) | Control group (n=32) | OR | 95%CI (confidenceinterval) | χ2 | р | ||
|---|---|---|---|---|---|---|---|---|
| Аbs. | % | Аbs. | % | <0,001* | ||||
| 18-24 | 4 | 6,3 | 5 | 15,7±6,5 | 0,92 | 1,28-3,02 | 0,02 | 0,920 |
| 25-29 | 28 | 43,8±6,2 | 8 | 25,0±7,6 | 2,06 | 0,42-1,54 | 13,11 | 0,920 |
| 30-34 | 11 | 17,2±4,8 | 7 | 21,9±7,3 | 0,98 | 0,48-1,76 | 0,02 | 0,086 |
| 35-39 | 7 | 10,9±3,9 | 6 | 18,8±6,3 | 0,72 | 0,42-1,04 | 2,64 | 0,034* |
| 40-44 | 6 | 9,4±3,7 | 3 | 9,3±5,3 | 0,48 | 0,22-1,17 | 4,23 | |
| 55-65 | 8 | 12,4±4,2 | 3 | 9,3±5,3 | 0,42 | 0,16-1,21 | 4,23 | |
Women aged 25-29 years are significantly more likely to be infected with HPV-HR (OR=2.06; p<0.001), while at the age of 18-24 years, HPV infection is less common (OR=0.92; p=0.002). In other age groups, no statistically significant differences were recorded (p>0.05). When analyzing socio-demographic indicators, it was found that women with HPV infection more often had secondary rather than higher education (OR=1.58; p=0.001) and were unmarried (OR=1.12; p<0.001). Among bad habits, only alcohol consumption did not increase the risk of HPV infection (OR=1.01; p=0.002). Before identifying the clinical features of the course of the disease in patients of the main group with PVI, it is of interest to register anamnestic provoking factors (Table 2). At the same time, more than half of women (46/64; 71.9±5.6%) do not associate the development of this neoplastic process with any provoking factors, while the other part of women (18/64; 28.1±5.6%) indicates a combination of several provoking factors.
Table 2: Provoking factors in patients of the main group (n=64).
| Provoking factors | Main group (n=64) | |
|---|---|---|
| Аbs. | % | |
| Antibacterial drugsand local antiseptics | 11 | 17,2±4,8 |
| Easily digestible carbohydrates (sweet, starchyfoods) | 12 | 18,8±4,9 |
| Spicy andsalty foods | 13 | 20,3±5,1 |
| Alcohol consumption | 3 | 4,68 |
| Smoking, tobacco, alternative smoking mixtures | 2 | 3,12 |
| Change of sexual partner | 4 | 6,3 |
| Hormonal contraception | 6 | 9,4 |
| Spermicides | 5 | 7,81 |
Among the anamnestic factors contributing to the clinical manifestations of the pathological process, the most frequently mentioned were the use of antibacterial drugs and local antiseptics (17.2±4.8%), various changes in eating behavior: the use of easily digestible carbohydrates (sweet, starchy foods) (18.8±4.9%), spicy and salty foods (20.3±5.1%). At the beginning, when clinical features were identified, complaints were collected with an active survey. The clinical picture in the examined patients was either absent or, in most cases, not pronounced. Two clinical forms of human papillomavirus infection were identified in patients: latent (n=28; 43.6±6.2%) and subclinical forms (n=36; 56.4±6.2%) (Table 3).
Table 3: Clinical characteristics of patients with latent (n=28) and subclinical forms of human papillomavirus (n=36).
| Clinical signs | Latent forms(n=28) | Subclinical forms(n=36) | ||
|---|---|---|---|---|
| Abs. | % | Abs. | % | |
| Number of allocations: | ||||
| - scanty | 1 | 3,6 | 2 | 5,5 |
| - moderate | 25 | 89,3±5,9 | 30 | 83,3±6,1 |
| - abundant | 2 | 7,1 | 4 | 11,2±5,4 |
| Character of discharge: | ||||
| - mucous | 24 | 85,8±6,6 | 27 | 75,0±7,2 |
| -"milky" | 2 | 7,1 | 4 | 11,2±5,4 |
| -"purulent" | 2 | 7,1 | 5 | 13,8±5,8 |
| Complaints: | ||||
| itching,burning | 3 | 10,7±5,9 | 6 | 16,7±6,3 |
| - dysuria | 1 | 3,6 | 5 | 13,8±5,8 |
| Pathological process: | ||||
| -vulvovaginitis | 6 | 21,4±7,8 | 10 | 27,8±7,5 |
| - cervicitis | 5 | 17,8±7,3 | 21 | 58,4±8,2 |
In 89.3±5.9% of patients (25/28) of latent and 83.3±6.1% of patients (30/36) of subclinical forms, complaints of moderate pathological leucorrhoea were detected, 10.7±5.9% ( 3/28) and 16.7±6.3% (6/36) experienced subjective sensations in the form of itching, burning, 3.6% (1/28) and 13.8±5.8% (5/36) dyspareunia. At the same time, the objective clinical picture often did not correspond to the complaints. Thus, during a gynecological examination, clinical signs of vulvovaginitis were found in 21.4±7.8% (6/28) of patients with latent and 27.8±7.5% (10/36) of patients with subclinical forms of papillomavirus infection. Inflammatory changes in the cervix (cervicitis) were detected in the majority of patients with subclinical forms of papillomavirus infection - 58.4±8.2% (21/36); with latent forms, cervicitis was detected in 17.8±7.3% (5/28) cases.
All patients underwent extended colposcopy. In patients with subclinical forms of PVI, changes in the mucous membranes of an inflammatory nature were found, characteristic of specific vaginitis and cervicitis (mild hyperemia of the vaginal mucosa, wavy surface over a large area of the epithelium of the cervix and vagina) (Table 4).
Table 4: Colposcopy in patients with various forms of PVI.
| Colposcopic results | Latent forms(n=28) | Subclinical forms(n=36) | Р | ||
|---|---|---|---|---|---|
| Аbs. | % | Аbs. | % | ||
| Acetowhite squamous epithelium | 4 | 14,4±6,7 | 13 | 36,1±8,0 | <0,001 |
| Condylomas acuminata | 2 | 7,1 | 6 | 16,7±6,3 | >0,05 |
| Flat condylomas | 5 | 17,8±7,3 | 12 | 33,3±7,8 | <0,001 |
| Punctuation | 3 | 10,7±5,9 | 9 | 25,0±7,2 | <0,001 |
| Mosaic | 2 | 7,1 | 6 | 16,7±6,3 | <0,05 |
| Iodine-negative epithelium | 5 | 17,8±7,3 | 11 | 30,6±7,7 | <0,001 |
| Atypical vessels | 4 | 14,4±6,7 | 8 | 22,2±6,9 | <0,001 |
| Erosion | 3 | 10,7±5,9 | 4 | 11,2±5,2 | <0,001 |
| Inflammation | 6 | 21,4±7,8 | 10 | 27,8±7,5 | <0,001 |
| Polyp | 1 | 3,6 | 3 | 8,3 | >0,05 |
In patients with latent forms of PVI, accordingly, such changes in the mucous membranes were absent. It is characteristic that in 47.22% (17/36) of patients with subclinical forms, manifestations of PVI were diagnosed both in the transformation zone and outside it (in the vaginal vault, on the vaginal walls, vulva). In all patients with latent forms of PVI, cytological examination did not reveal specific changes in the mucous membranes of the lower genitalia. In some cases, an inflammatory reaction was detected (21.4±7.8%), in 14.4±6.7% of patients acetowhite squamous epithelium was found, in 14.4±6.7% of cases atypical vessels were detected and in 10. Erosion was detected in 7±5.9% of cases.
A comparative analysis of cytomorphometric study data showed that to determine cellular changes in HPV, the most reliable differential diagnostic criteria are: 1) number of koilocytes, 2) parakeratosis, 3) squamous metaplasia. The possibility of clarifying the diagnosis of HPV-associated subclinical lesions of the lower genitalia is achieved by histological examination of biopsy samples of the affected areas. The following morphological signs of PVI were assessed: - in the surface epithelial cells the presence of koilocytes - vacuolization of the cytoplasm against the background of hyperchromia and pyknosis of the nuclei, as well as basal cell hyperplasia, thickening of varying degrees of multilayered squamous epithelium with signs of hyper-, para-, and acanthosis of the underlying tissues, as well as phenomena chronic inflammatory infiltration. The main cytological sign of HPV damage to the epithelium is the presence of specific cells-koilocytes, mentioned in the publications of some authors [6,8]. When conducting a histological examination of scrapings of the walls of the vagina, exo- and endocervix, koilocytic cell atypia was revealed in patients with subclinical forms of PVI (86.1% (31/36), among other cellular elements neutrophilic leukocytes (75.0%), lymphocytes (19.4%). The remaining changes characteristic of HPV lesions of the lower genitalia were minimal (Figure 1).
Depending on the localization of the smear material and the presence of a transformation zone, the smears also contained unchanged cells of stratified squamous epithelium, metaplastic, basal/parabasal cells and columnar epithelial cells, indicating chronic inflammation, confirmed by data from other authors [8-10].
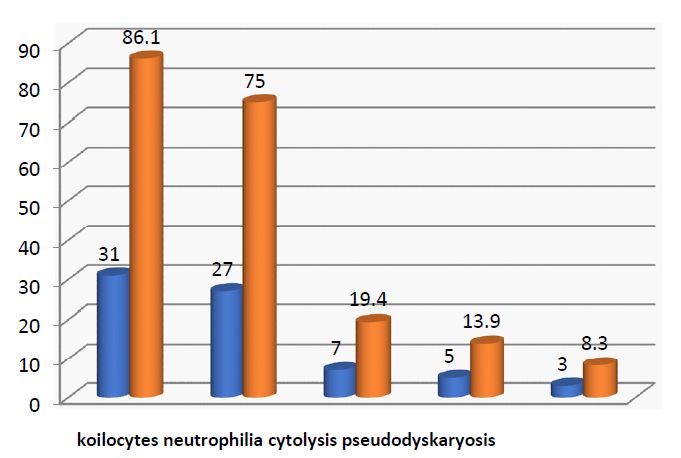
Figure 1: Cytological characteristics of epithelial lesions of the lower genitalia of patients with subclinical forms of PVI (n=36).
In order to prevent PVI, 20 women in the control group were vaccinated with the Gardasil-4 Vaccine, which protects against four types of papillomavirus: 16, 18 (similar to the Cervarix vaccine), as well as 6, 11, which cause genital warts. Vaccination was administered to 5 women (15.7±6.5%) aged 18-24 years, 8 women (25.0±7.6%) aged 25-29 years and 7 women (21.9±7.3%) aged 30-34 years. This vaccine is quite easily tolerated, does not cause fever, and does not lead to infertility. Vaccination was carried out according to the scheme 0-2-6 months.
The conducted surveys show that it is important to properly organize explanatory work on the organization and conduct of examinations of women for HPV. There are two systems of cytological screening for cervical cancer: organized (systematic) screening and unorganized (sporadic) screening. During organized screening, the contingent of women to be screened is determined, its frequency is determined, and women are actively invited to participate in the examination. During unorganized screening, only women who have applied to medical institutions for any reason are examined. Our data are consistent with previous studies by many authors reporting that systematic screening is more effective than sporadic screening [11,12]. HPV belongs to the group of oncological diseases that fully meet the requirements of population screening.
Conclusion
1. The data obtained during the study show the multisystem nature of the identified disorders that occur during PVI infection and indicate the presence in patients with subclinical forms of human papillomavirus infection of medical and social factors that create an unfavorable premorbid background and cause the transition of the infection from the subclinical form to the clinical one.
2. Due to the widespread spread of the human papillomavirus in recent years, its socio-economic significance and the insufficient volume of preventive measures taken for this disease, an increase in the level of infection of women with this infection has been observed.
3. With widespread screening coverage of the female population and the use of effective treatment methods, as well as thanks to HPV vaccination, the incidence of PVI can be reduced to 95%.
References
- Aliev DA, Mardanly FA. i dr. Epidemiologicheskie aspekty zlokachestvennyh novoobrazovanij v Azerbajdzhanskoj Respublike za 2008-2013 g.// Azərbaycan Onkologiya J. 2014; 2: 32-38.
- Chesson HW, Unger ER, Romero JR, Markowitz LE. Human рapillomavirus vaccination for adults: Updated recommendations of the advisory committee on immunization practices. MMWR Morb Mortal Wkly Rep. 2019; 68: 698-702. doi:10.15585/mmwr.mm6832a3 pmid:31415491
- Ng SS, Hutubessy R, Chaiyakunapruk N. Systematic review of cost-effectiveness studies of human papillomavirus (HPV) vaccination: 9-Valent vaccine, gender-neutral and multiple age cohort vaccination. Vaccine 2018; 36: 2524-doi:10.1016/j.vaccine.2018.03.024 pmid:29625764
- Khryanin AA, Tapil’skaya NI, Knorring GYu. Modern concepts of human papillomavirus infection: Epidemiology and treatment tactics of patients with ano-genital warts. Russian Journal of Clinical Dermatology and Venerology = Klinicheskaya dermatologiya i venerologiya. 2020; 19(5): 719-728. https://doi.org/10.17116/klinderma202019051719
- Briko NI, Sekacheva MI, Lopukhov PD, Kobzev GS, Kaprin AD, et al. Clinical and epidemiological features of manifestations of papillomavirus infection on the example of cervical cancer and anogenital (venereal) warts. Vestnik of the Russian Academy of Medical Science. 2020; 75(1): 77-82. (In Russ.).
- Bergman H, Buckley BS, Villanueva G, et al. Comparison of different human papillomavirus (HPV) vaccine types and dose schedules for prevention of HPV-related disease in females and males Cochrane Gynaecological, Neuro-oncology and Orphan Cancer Group, Cochrane Database Syst Rev. 2019; 2019(11): CD013479. Published online 2019 Nov 22.
- Lawson JS, Glenn WK. Evidence for a causal role by human papillomaviruses in prostate cancer- a systematic review. Infect Agents Cancer. 2020; 15: 41. https://doi.org/10.1186/s13027-020-00305-8
- Nejo YT, Olaleye DO, Odaibo GN. Prevalence and Risk Factors for Genital Human Papillomavirus Infections Among Women in Southwest Nigeria. Arch Basic Appl Med. 2018; 6(1): 105-112.
- De Oliveira СМ, T G Fregnani JH, Villa LL. HPV Vaccine: Updates and Highlights. Acta Cytological. 2019; 1-10. Doi: 10.1159/000497617.
- MacLaughlin KL, Jacobson RМ, Breitkopf CR, Wilson PМ, Jacobson DJ, et al. Trends Over Time in Pap and Pap-HPV Cotesting for Cervical Cancer Screening. J Womens Health (Larchmt). 2019; 28(2): 244-249. Epub 2019 Jan 7. Doi: 10.1089/ fwh.2018.7380.
- Del Prete, Ronga L, Magrone R, Addati G, Abbasciano A, et al. Epidemiological evaluation of human papillomavirus genotypes and their associations in multiple infections. Epidemiology and Infection. 2019; 147. doi: 10.1017/S0950268818003539.
- Bocharova II, Zarochentseva NV, Vlasova VA, Aksenov AN, Belaya YuM, et al. The effect of maternal papillomavirus infection on the health of the newborn. Russian Bulletin of Obstetrician-Gynecologist = Rossiiskii vestnik akusheraginekologa. 2020; 20(4): 82-87. (In Russ.). https://doi.org/10.17116/rosakush20202004182
