
Open Access, Volume 10
Conservative management of a mandibular parasymphysis and body fracture with arch bar fixation in a pediatric patient
Srushti Akulwar*; Abhilasha Agarwal; Rajeev Kumar Singh; Richa Khanna
Department of Paediatric and Preventive Dentistry, Faculty of Dental Sciences, King George Medical University, U.P., Lucknow, India.
Srushti Akulwar
Department of Paediatric and Preventive Dentistry, Faculty of Dental Sciences, King George Medical University, U.P., Lucknow, India.
Phone/Fax: +39-336-945902; Email: arturogiordano@tin.it
Received : July 02, 2024,
Accepted : July 26, 2024
Published : July 30, 2024,
Archived : www.jclinmedcasereports.com
Abstract
A pediatric mandible fracture is one of the most challenging scenarios to manage in maxillofacial trauma. Pediatric mandible fracture management requires consideration of age, dental and skeletal developmental stage, fracture site, and the extent of the patient’s cooperation with the suggested treatment. Although the causes of mandibular fractures in children may be varied, the symptoms are often the same as in adults. The treatment principles for mandibular fractures differ from those of adults due to concerns regarding mandibular growth and the development of dentition. The main objective is to restore the underlying bony architecture to its pre-traumatic state as conservatively as possible with minimal functional impairment. A girl of around 5 years with a fractured mandibular body and contralateral parasymphysis fracture managed by closed reduction and short-term immobilization with an arch bar under local anesthesia is presented.
Keywords: Immobilization; Mandibular fractures; Paediatric; Trauma.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Akulwar S (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Akulwar S, Agarwal A, Singh RK, Khanna R. Conservative management of a mandibular parasymphysis and body fracture with arch bar fixation in a pediatric patient. Open J Clin Med Case Rep. 2024; 2269.
Introduction
Children experience maxillofacial trauma less frequently than adults (0.6%-1.2%) [1]. Mandibular fractures account for 36% of all facial fractures in pediatric patients. About 80% are angle, condyle, and sub-condyle fractures, and the rest, about 15-20%, are symphysis and parasymphysis fractures [2]. Due to the elasticity of the mandible, embedded tooth buds holding the fragments together, and short condylar neck, most of the body and symphysis fractures in children are undisplaced, which can be managed conservatively [3].
The management for pediatric mandible fractures concentrate on minimizing aesthetic and functional impairment, achieving stability without invasive treatments, and returning the underlying bone architecture to its pre-injury position [4]. Closed reduction and immobilization are conservative, non-invasive treatment options for mandibular fractures, when compared to open reduction and internal fixation [3]. An unexpected effect on growth may occur from disruption of the mandibular body’s periosteal envelope. To overcome this, the closed reduction and immobilization technique is preferred for minimally displaced fractures [5].
Proper guidelines for intermaxillary fixation in the pediatric age group are nonexistent, and pervasive dogma, often argues against conventional arch bars in pediatric patients during primary and mixed dentition. However, no objective data supports these theories, with the literature demonstrating that arch bars can be safely used in children with no periodontal defects, tooth avulsions, or disturbances to permanent dentition [6,7]. Erich arch bars prevent the insult of open reduction and internal fixation promotes the precise reduction and stabilization of the mandibular fractures [8].
The treatment in the present case aimed to achieve bony union, normal occlusion, form, and function, and to avoid impediments to normal growth. To achieve this, arch bar fixation, using firm primary teeth as anchors, was planned to correct the minimally displaced, unfavorable mandibular fracture.
Case Presentation
A young girl reported to the Department of Pediatric and Preventive Dentistry with the chief complaint of pain and swelling in the lower jaw. The patient had a history of falling from height while playing 10 days ago. The history of unconsciousness, vomiting, ENT bleeds, and convulsions after the fall was negative. The patient went to a local hospital, but no intervention was done. The extra-oral examination revealed a diffuse swelling over the bilateral lower one-third of the face, which was tender on palpation. Lacerations were present over the chin region on palpation, associated with deranged occlusion leading to the appearance of an open mouth (Figure 1A). On palpation, step deformity and tenderness were noted over the left parasymphysis region and the lower border of the jaw. An intraoral examination indicated a gap in the tooth left mandibular canine and primary first molar regions. Teeth were not in proper occlusion and slight midline deviation was seen. Multiple carious teeth were present (Figure 1B).
Investigations
The provisional diagnosis was a combined fracture of the left para symphysis associated with a right mandibular body, and Cone beam computed tomography (CBCT) was suggested to confirm it. The Orthopantogram (OPG) and Cone beam computed tomography (CBCT) preoperatively confirmed left para symphysis fracture with a step at the inferior border of the mandible. An associated minimally displaced fracture was present on the right mandibular body region (Figures 2,3). Routine hematological investigations were advised, and emergency treatment was started. Meanwhile, antibiotics and analgesics were prescribed, along with a dose of tetanus toxoid injection. Intravenous fluids were also prescribed since the child was unable to take food orally.
Treatment
After a thorough clinical and radiographic examination, it was planned to manage the condition using the non-surgical closed reduction technique of Inter-Maxillary Fixation (IMF). Fractured fragments were reduced under local anesthesia (2% Lidocaine with 1:200000 adrenaline) and chairside sedation with Midazolam (0.5 mg/kg) (Mezolam - Neon Laboratories Ltd.). Prestretched 26-gauge stainless steel wire at the optimum lengths for the maxilla and mandible was used to secure the pediatric arch bars. Elastics (Blue, 1/4”-3.5 Oz) were placed to secure occlusion, as they are assumed to be better tolerated in children with equivalent outcomes of fracture healing and mandibular function (Figure 4A, 4B). The patient was kept on a soft diet, oral hygiene instructions were given and analgesics were prescribed.
Outcome and follow-up
In the second post-operative week, IMF was removed, no mobility was present at the fracture site, and occlusion was satisfactory. At one month follow-up, clinical examination revealed satisfactory occlusion (Figure 5A). The carious teeth were restored with restorative glass ionomer cement (GC Fuji II) and light cure composite (3MTM FiltekTM Universal restorative) (Figure 5B). Radiographic presentation on one-month follow-up revealed complete healing of the fracture site (Figure 6). Postoperative recovery was uneventful, and the patient was reviewed monthly for 6 months (Figures 7,8).

Figure 1: (A) Profile photograph showing lacerations over chin and open bite appearance. (B) Intraoral photograph showing deranged occlusion and gap between left mandibular primary canine and first molar region.

Figure 2: Preoperative orthopantomogram (OPG) reveals right mandibular body and left mandibular para symphysis fracture.
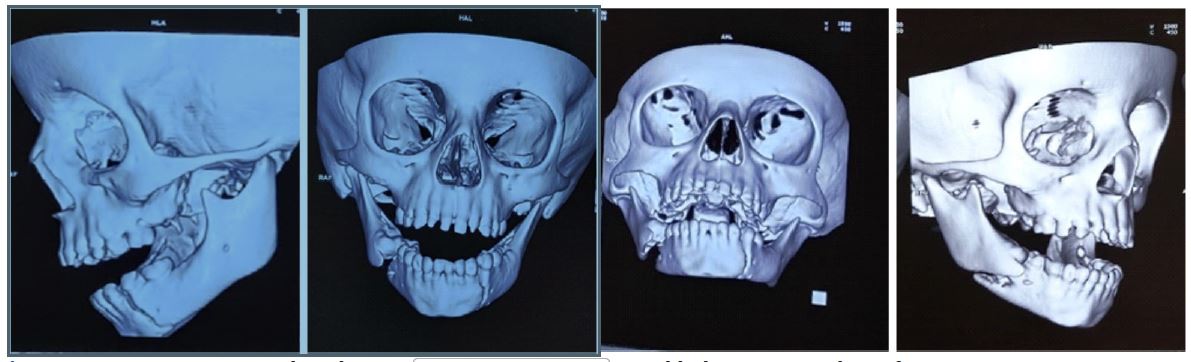
Figure 3: CBCT 3D view reveals right mandibular body and left mandibular para symphysis fracture.
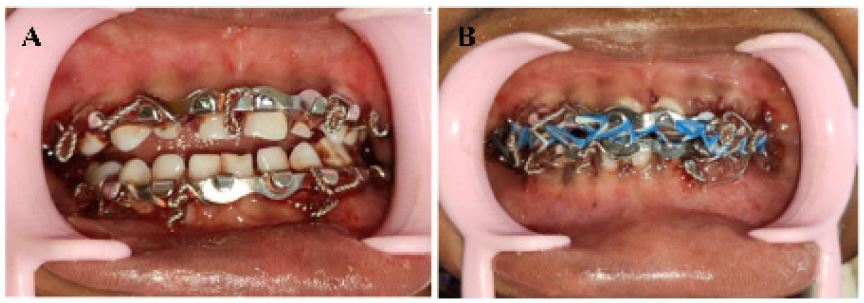
Figure 4: (A-B) Intra-oral photograph after the Arch bar fixation.

Figure 5: (A) Intraoral photograph showing satisfactory occlusion at 1-month follow-up.
(B) Post-operative intraoral photograph after restorations.
(B) Post-operative intraoral photograph after restorations.

Figure 6: Post-operative orthopantomogram (OPG) at 1-month follow-up reveals a bony union of the right mandibular body and left mandibular para symphysis fracture.
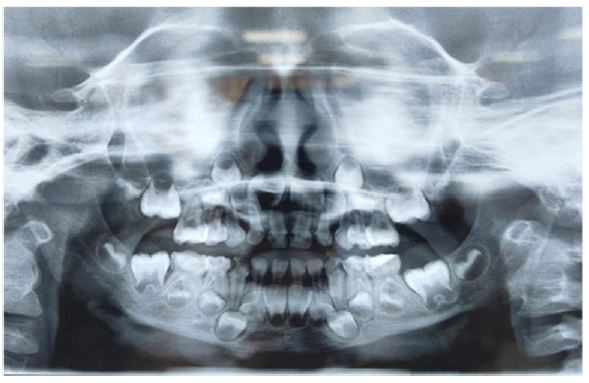
Figure 7: Post-operative orthopantomogram (OPG) at 6 months follow-up showing complete healing of the fracture site.
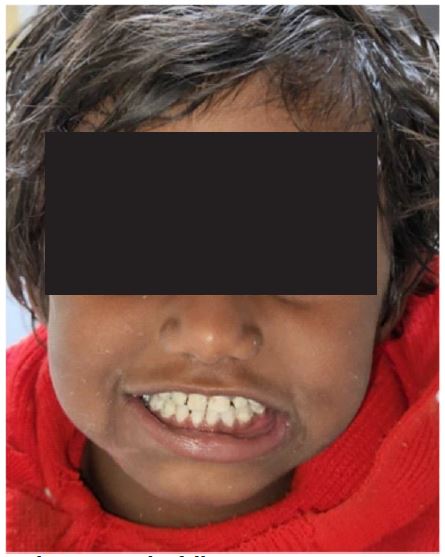
Figure 8: Post-operative profile photograph at 6 months follow-up.
Discussion
Facial fractures in pediatric and adult populations vary, with nasal bone fractures being the most common in adults and mandible fractures in children due to differential growth patterns. The most common causes of mandibular fractures in children are sports injuries, falls from a height, accidents, and child maltreatment [9,10]. Literature suggests that condylar fractures (31-45%) are more common in young children than para symphysis fractures (13-26%) because of the highly vascular pediatric condyle, thin cortices, and less resistant medullary bone against impact forces [11-13].
The type of fracture and the stage of dental and skeletal development determine the way pediatric mandibular fractures are managed. The development of the dentition and mandible growth are the primary concerns while managing such fractures. The majority of pediatric fractures are ‘greenstick’ type, where close observation, a liquid-to-soft diet, and analgesics during the healing phase are advised [14,15]. Though treatment alternatives such as closed reduction with intermaxillary fixation and open reduction with various fixation methods exist, the use of mini-plates in children may be limited due to the risk of interference with ongoing dental development. Resorbable plates offer an alternative but carry the potential for tooth bud damage [5]. The open reduction management technique is not considered due to incomplete ossification of the mandible and underlying erupting teeth. Reduced surgical trauma to the patient, a decreased risk of iatrogenic injury to developing teeth and other anatomical structures, and cost-effectiveness are the benefits of closed reduction over open reduction [9]. Furthermore, the rate of associated complications is lower in cases of closed reduction compared to open reduction [5].
Cap splints, prefabricated occlusal splints, lingual splints, circumferential wiring, arch bars, or gunning splints are some of the various closed reduction and immobilization treatment techniques available for the management of pediatric mandible fractures [5,14]. These techniques offer periosteal sleeve continuity as well as a good reduced position. They also preserve the soft tissue and establish a favorable environment for quick osteogenesis and remodeling processes, thus preventing non-fibrous bony union [15,16]. It is desirable to minimize the period of immobilization to not more than 2-3 weeks for young patients due to their high potential for healing, high osteogenic capacity of the periosteum, and high metabolic rate of developing tissue [17].
Several studies have recommended the use of cap splints as a treatment for pediatric mandibular fractures [18,19]. These splints are more reliable than open reduction or IMF techniques concerning cost-effectiveness, ease of application and removal, reduced operating time, maximum stability during the healing period, minimal trauma for adjacent anatomical structures, and comfort for young patients. Furthermore, in the splinted mandible, the fracture segments are tightly fixed and serve to reduce tenderness and pain reactions during a child’s daily activity [20]. However, in cases of displaced body mandibular fracture, this approach may be insufficient, and healing might get prolonged due to the poor compliance of young patients with postoperative instructions. To overcome this, intermaxillary fixation with arch bars under chairside sedation and local anesthesia was planned in the present case to maintain stability and achieve the pre-traumatic state. Arch bars are an important component of adult mandible fracture management; however, their use has been controversial in patients during primary and mixed dentition19. Literature has illustrated the safe and efficacious use of arch bars in patients during primary and mixed dentition, which yielded uncompromised dental health at follow-up, with specifically no periodontal defects, tooth avulsions, or disturbances to permanent dentition [7].
Conclusion
In the present case, the authors have successfully managed the combination mandibular fracture by performing intermaxillary fixation without need for open reduction or surgical intervention. Follow-up appointments were scheduled at regular intervals to monitor the healing progress and skeletal and dental development.
Declarations
Author contributions: S Akulwar and Agarwal A: Conceptualization and Data curation; Writing – original draft. R Khanna: Supervision. RK Singh and R Khanna: Writing - review and editing. All authors read and approved the final manuscript.
Acknowledgments: Our heartfelt gratitude goes to the patient and her family for their consent, support, and cooperation during treatment.
Conflict of interest statement: None declared. We hereby declare that there is no conflict of interest regarding the publication of this paper, and we declare that the information given is true to the best of our knowledge.
Funding information: No funding was declared.
Acknowledgments: Our heartfelt gratitude goes to the patient and her family for their consent, support, and cooperation during treatment.
References
- Das UM, Nagarathna C, Viswanath D, Keerthi R, Gadicherla P. Management of facial trauma in children: A case report. Journal of Indian Society of Pedodontics and Preventive Dentistry. 2006; 24(3): 161-3.
- Boffano P, Roccia F, Zavattero E, Dediol E, Uglešić V, et al. European Maxillofacial Trauma (EURMAT) in children: A multicenter and prospective study. Oral surgery, oral medicine, oral pathology and oral radiology. 2015; 119(5): 499-504.
- Mulliken JB, Kaban LB, Murray JE. Management of facial fractures in children. Clinics in Plastic Surgery. 1977; 4(4): 491-502.
- Moss ML, Rankow RM. The role of the functional matrix in mandibular growth. The Angle Orthodontist. 1968; 38(2): 95-103.
- Aizenbud D, Hazan‐Molina H, Emodi O, Rachmiel A. The management of mandibular body fractures in young children. Dental traumatology. 2009; 25(6): 565-70.
- Farber SJ, Nguyen DC, Harvey AA, Patel KB. An alternative method of intermaxillary fixation for simple pediatric mandible fractures. Journal of Oral and Maxillofacial Surgery. 2016; 74(3): 582-e1.
- Naran S, Keating J, Natali M, Bykowski M, Smith D, et al. The safe and efficacious use of arch bars in patients during primary and mixed dentition: A challenge to conventional teaching. Plastic and Reconstructive Surgery. 2014; 133(2): 364-6.
- Stacey DH, Doyle JF, Mount DL, Snyder MC, Gutowski KA. Management of mandible fractures. Plastic and reconstructive surgery. 2006; 117(3): 48e-60e.
- Kaban LB. Diagnosis and treatment of fractures of the facial bones in children 1943–1993. Journal of oral and maxillofacial surgery. 1993; 51(7): 722-9.
- Posnick JC, Wells M, Pron GE. Pediatric facial farctures: Evolving patterns of treatment. Journal of oral and maxillofacial surgery. 1993; 51(8): 836-44.
- Haug RH, Foss J. Maxillofacial injuries in the pediatric patient. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 2000; 90(2): 126-34.
- Glazer M, Joshua BZ, Woldenberg Y, Bodner L. Mandibular fractures in children: analysis of 61 cases and review of the literature. International journal of pediatric otorhinolaryngology. 2011; 75(1): 62-4.
- Ferreira PC, Amarante JM, Silva ÁC, Pereira JM, Cardoso MA, et al. Etiology and patterns of pediatric mandibular fractures in Portugal: A retrospective study of 10 years. Journal of Craniofacial Surgery. 2004; 15(3): 384-91.
- Zimmermann CE, Troulis MJ, Kaban LB. Pediatric facial fractures: recent advances in prevention, diagnosis and management. International journal of oral and maxillofacial surgery. 2005; 34(8): 823-33.
- Rowe NL. Fractures of the jaw in children. J. oral Surg. 1969; 27: 497-507.
- Tanaka N, Uchide N, Suzuki K, Tashiro T, Tomitsuka K, et al. Maxillofacial fractures in children. Journal of Cranio-Maxillofacial Surgery. 1993; 21(7): 289-93.
- Sharma A, Patidar DC, Gandhi G, Soodan KS, Patidar D. Mandibular fracture in children: A new approach for management and review of literature. International journal of clinical pediatric dentistry. 2019; 12(4): 356.
- Kumar N, Gauba K. Modified closed cap splint: Conservative method for minimally displaced pediatric mandibular fracture. The Saudi dental journal. 2018; 30(1): 85-8.
- Kale TP, Urologin SB, Kapoor A, Lingaraj JB, Kotrashetti SM. Open cap splint with circummandibular wiring for management of pediatric mandibular parasymphysis/symphysis fracture as a definitive treatment modality; a case series. Dental Traumatology. 2013; 29(5): 410-5.
- Smartt Jr JM, Low DW, Bartlett SP. The pediatric mandible: II. Management of traumatic injury or fracture. Plastic and reconstructive surgery. 2005; 116(2): 28e-41e.
