
Open Access, Volume 10
Peribiliary cysts in a normal liver: Case report and review of the literature
Anna Stegmann1; Karla Scamardi2; Jürg Vosbeck3; Savas D Soysal2; Otto Kollmar2; Gabriel F Hess2
1Charité - Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany.
2Clarunis, Department of Visceral Surgery, University Center for Gastrointestinal and Liver Diseases, St. Clara Hospital and University Hospital Basel, Switzerland.
3Institute of Medical Genetics and Pathology, University Hospital Basel, Basel, Switzerland.
Gabriel F Hess
Clarunis University Center for Gastrointestinal and Liver Disease, St. Clara Hospital and University
Hospital Basel, Spitalstrasse 21, CH-4056, Basel, Switzerland.
Email: gabriel.hess@clarunis.ch
Received : July 05, 2024,
Accepted : July 25, 2024
Published : July 31, 2024,
Archived : www.jclinmedcasereports.com
Abstract
A 72-year-old female presented with acute epigastric pain, vomiting and fever. She was diagnosed with a cholangiosepsis caused by Escherichia coli. In the past few years, she had been hospitalized multiple times due to recurrent cholangitis. Ten years earlier, magnetic resonance imaging had incidentally revealed a stricture of the left bile duct, accompanied by poststenotic dilatation and small cysts in the surrounding area. Brush cytology showed no carcinoma, there was no progression in regular ultrasound examination and the patient remained asymptomatic for several years. Subsequent cholelithiasis and recurrent cholangitis were treated with antibiotics and elective cholecystectomy.
When she presented with cholangiosepsis this time, surgical therapy was indicated due to persisting obstructive symptoms and the inability to definitively exclude an obstructive tumor. Histology showed several peribiliary cysts causing a stricture of the left bile duct. These so-called “Nakanuma cysts” should be considered as a possible cause for bile duct obstruction, recurrent cholangitis and cholangiosepsis.
Keywords: Peribiliary cysts; Nakanuma; Cholestasis; Cholangiosepsis; Caroli’s disease; Cholangiocarcinoma.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Hess GF (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Stegmann A, Scamardi K, Vosbeck J, Soysal SD, Kollmar O, et al. Peribiliary cysts in a normal liver: Case report and review of the literature. Open J Clin Med Case Rep. 2024; 2268.
Introduction
Peribiliary cysts were first described by Nakanuma et al. in 1984 as cystic dilatation of the intrahepatic extramural, peribiliary glands around the intrahepatic large bile ducts [1]. These lesions develop usually around the hepatic hilum, measuring < 20 mm in diameter and lacking communication with the adjoining large bile ducts [2]. They can at times cluster together resembling a multilocular malignancy, mimic biliary dilatation or grow to compress the neighbouring structures, resulting in obstruction of the biliary tree, consequently causing cholestasis or cholangitis [2-4].
Usually asymptomatic, peribiliary cysts are benign lesions generally found incidentally on diagnostic imaging studies [3,5]. These cysts often occur in patients with advanced liver diseases, particularly liver cirrhosis or disturbances of the portal venous system and in rare cases they may be present in patients with history of alcohol abuse or without any underlying hepatic diseases [4,6-8].
The clinical significance of these structures lies in their potential to mimic other diseases. It is crucial to distinguish peribiliary cysts from premalignant conditions or malignant cystic lesions [8,9]. The following case illustrates peribiliary cysts causing recurrent biliary obstruction, cholangitis and ultimately cholangiosepsis in a patient with a non-cirrhotic liver.
Case Presentation
A 72-year-old white female patient with a history of Systemic Lupus Erythematosus (SLE) and secondary Sjögren’s Syndrome (SjS) recently presented in our hospital with acute epigastric pain, nausea, vomiting, fever, chills and dark brown urine. Her clinical findings included elevated blood inflammation markers and altered liver and cholestatic parameters, suggesting infection and obstruction. Over the past few years, the patient had been hospitalized multiple times for recurrent cholangitis. Currently a cholangiosepsis caused by Escherichia coli was diagnosed.
Ten years prior, she had been hospitalized with an inflammatory myopathy diagnosed as a polymyositis, likely related to SjS. To rule out a neoplastic aetiology, a magnetic resonance imaging (MRI) of the abdomen was performed. The MRI coincidentally revealed a 20 mm stricture of the left bile duct with a poststenotic dilatation and multiple small cysts in the vicinity (Figure 1). The right bile duct and the common hepatic duct were not involved. The stricture was suspicious to be caused by a hilar cholangiocellular carcinoma, also termed as Klatskin tumor. An Endoscopic Retrograde Cholangiopancreatography (ERCP) including papillotomy confirmed the segmental stricture and poststenotic dilatation of the left bile duct, suggesting malignancy, but brush cytology showed no carcinoma. Unfortunately, the patient developed an iatrogenic duodenal perforation and an infected retroperitoneal hematoma as complications from the ERCP. She was treated with antibiotics, recovered well, and the hematoma resolved over the following months.
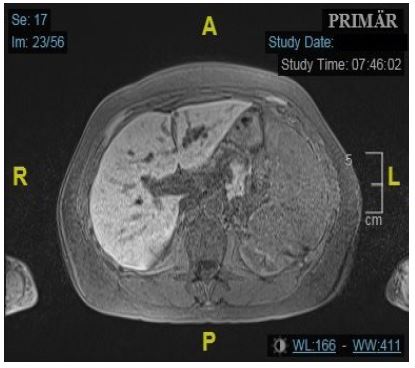
Figure 1: Axial T1w-fs MRI: First observati on of stenotic left bile duct and additional cystic formations.
Over the following years, the patient remained asymptomatic, with regular ultrasounds showing no progression of the left biliary duct dilatation. After six years, the patient was hospitalized with acute cholecystitis due to cholelithiasis. An abdominal Computer Tomography (CT) scan revealed a gallbladder wall thickening with a stone in the infundibulum and the known left bile duct dilatation. The serum CA 19-9 was elevated at 640.4 U/ml (reference: < 37 U/ml). A conservative management of the cholecystitis with antibiotics was employed and the patient was subsequently discharged without any symptoms. Two months later, the patient was readmitted with cholangiosepsis by Escherichia coli. CT and Magnetic Resonance Cholangiopancreatography (MRCP) showed no progression of the left bile duct stricture and dilatation (Figure 2). MRCP presented an echo-rich formation around the left hilum (sludge), suggesting cholangitis, but no signs of choledocholithiasis or alterations in the liver parenchyma. An ultrasound examination of the abdomen confirmed those findings. The patient underwent an early elective cholecystectomy. The gallbladder histology showed no malignancy. At this timepoint, a diagnosis of cholangiocellular carcinoma was deemed unlikely due to the absence of lymphadenopathy and consistent clinical and radiological findings.

Figure 2: Coronar T2w MRCP: Known dilatation of the left bile duct during first episode of cholangitis.
After cholecystectomy, the patient initially remained asymptomatic. However, four years later, she experienced two episodes of recurrent cholangitis, with a six-month interval in between them, the latter complicated by cholangiosepsis. During the first episode, surgical intervention was considered due to obstructive symptoms and recurrent cholangitis. Despite the absence of significant pathological findings and clear evidence on ERCP, MRI and CT, an obstructive tumor could not be definitively excluded. The surgery was postponed due to the SARS-CoV-2 pandemic.
In the second episode, the patient presented septical, with low blood pressure and tachycardia. Elevated cholestatic parameters and liver enzymes were noted, in addition Escherichia coli was found in blood cultures again. CT showed progression of the left bile duct dilatation and an additional enlargement of the common bile duct. MRCP confirmed those findings and for the first time, concretions inside the enlarged left duct and cystic expansions were observed (Figures 3 & 4). SLE was considered as a possible cause of hepatopathy, but antibody diagnostics were negative, and there were no signs of SLE activity. Viral infections were ruled out and the patient had no history of liver disease or alcohol abuse.
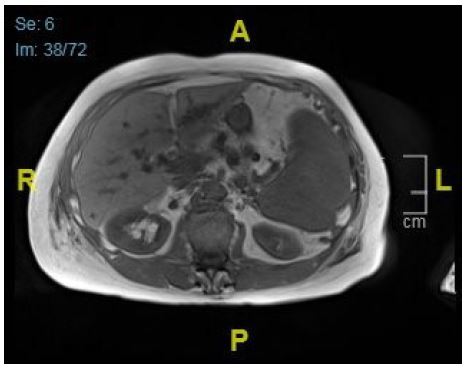
Figure 3: Axial T1w-dixon MRI: Progression of cystic formations in the left liver lobe.
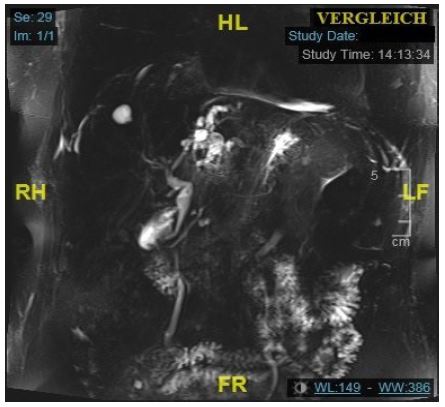
Figure 4: Coronar T2w-MRCP shows stricture of the left bile duct measuring 20 mm and a poststenotic curved dilatation with multiple concretions. DHC is enlarged as well.
After one week of antibiotic therapy the patient was stable enough to undergo hepatectomy. The procedure involved the anatomic resection of segments I, II, III and a lymphadenectomy. During the resection, a cyst measuring 15 mm connected with segment I was found. Thus, an anatomic resection of segment I was performed as well. Intraoperative frozen sections demonstrated no carcinoma, but the cyst was suspicious for an Intraductal Papillary Mucinous Neoplasm (IPMN).
The patient’s postoperative recovery was rapid and free of complications. Inflammatory markers and liver enzymes normalized. Intrabdominal drainages delivered little serous exudate and were removed on the second postoperative day. The bowels movements were regular and a normal could be started two days after operation. The patient was discharged eight days after surgery without any complications

Figure 5: Coronar Macroscopic resection specimens of liver segments I, II and III.
Histology of the surgical specimen revealed surprising findings: There was no evidence of neoplasia. However, several peribiliary cysts, so called “Nakanuma cysts”, could be identified (Figure 5), including one large extrahepatic cyst (Figure 6), and multiple smaller cysts (Figure 7) in the left lobe, causing stricture of the left bile duct with consecutive cholestasis, hepatolithiasis and cholangitis leading to cholangiosepsis.
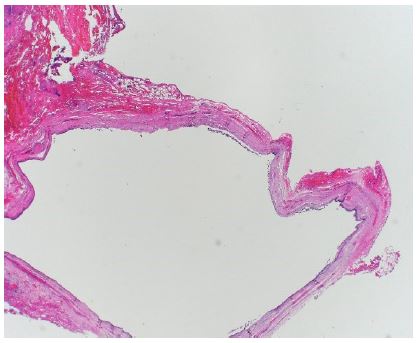
Figure 6: Microscopic image of extrahepatic cyst.
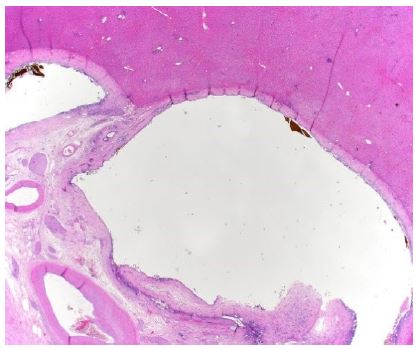
Figure 7: Microscopic image of intrahepatic peribiliary cysts.
Discussion
Terada and Nakanuma analysed 1000 consecutive autopsy livers and found cystic alterations of the peribiliary glands in 20.2% [4]. The aetiology of peribiliary cysts remains unknown and at least two different pathogeneses have been proposed [10]: Firstly, peribiliary cysts are reported in 1% of the pathology of explanted livers, but they have a prevalence of 66% in patients with Autosomal Dominant Polycystic Kidney Disease (ADPKD) and up to 100% in autopsies of patients with Autosomal Dominant Polycystic Liver Disease (ADPLD) [2]. In these cases, a hereditary component is considered, concerning PKD1 and PDK2 gene mutations, which lead to an impairment of the function of primary cilia involving the intrahepatic biliary tree and peribiliary glands [7,10,11]. Additional associated diseases include cirrhosis (38%), portal hypertension (34%), portal vein thrombosis (10%), hepatic, biliary or pancreatic neoplasms (17%) and primary sclerosing cholangitis (1.5%) [12]. In 15% of the cases, no associated conditions or diseases are present [2]. The second hypothesis involves a change in the microenvironment of the extramural peribiliary glands caused by various factors (e.g. alcohol, cirrhosis or portal hypertension) with inflammation and circulatory disturbance in advanced liver diseases [3,13].
Here we present a case of peribiliary cysts in a normal liver. The patient did not suffer from ADPLD, liver cirrhosis or portal hypotension, nor did she have a history of other liver diseases or alcohol abuses. Her pre-existing conditions included SLE and a SjS.
We found no case reports in the literature addressing the association of peribiliary cysts with SLE or SjS. Given the hypothesis of a change in the liver microenvironment, these systemic diseases could have influenced the development of the cysts. SLE may affect the liver and lead to fibrosis and cirrhosis, which are reported to be associated with peribiliary cysts. Literature describes liver involvement in rheumatic diseases, with a liver dysfunction in 20-43% of SLE patients. In SjS, liver dysfunction prevalence ranges from 7-34% , with 5% of these cases being caused by AIH or PBC [14]. However, our patient had no pre-existing liver condition, and histology of the non-cystic liver showed isolated minimal periductal fibrosis and low siderosis (Searle grade I) without any disease value. Although this is the first reported case of peribiliary cysts associated with SLE and SjS, further cases should be documented.
A systematic review of 135 patients revealed, that peribiliary cysts were multiple in 90% of cases and solitary in 10%. Cysts ranged from 1 to 55 mm in size and were found intrahepatic (87%), extrahepatic (7%) and rarely in both locations (6%) [2]. Based on this observation, Bazerbachi et al. developed a classification system for peribiliary cysts (Figure 8).
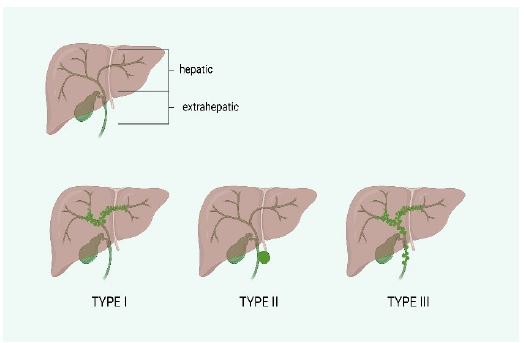
Figure 8: Classification framework for peribiliary cysts according to Bazerbachi et al. 2018. Type I: hepatic, type II: extrahepatic, type III: mixed hepatic and extrahepatic.
The pathology report of the liver specimen described intra- and extrahepatic cysts, consistent with type III of the classification. Type III cysts, with mixed locations, are rare and found in only 6% of patients [2]. Extrahepatic cysts are more frequent in women, often appear solitary, are not associated with cirrhosis or portal hypertension, and frequently present with obstructive jaundice, as in our patient [2].
In most cases, the cysts are asymptomatic and only few patients develop complications. Bile duct dilatation, obstructive jaundice and cholangitis are the most frequent complications [3,12,15-17]. Hepatolithiasis, acute pancreatitis and cysts infection are rare [2]. Asymptomatic peribiliary cysts are often found incidentally by imaging. Contrast-enhanced CT (CECT) and MRCP are the recommended imaging modalities. Drip infusion cholangiographic CT (DIC-CT), MRI with gadoxetic acid and ERCP can prove a lack of communication with the biliary tract, DIC-CT showed the highest accuracy [2,3,7,18].
Surgery is not generally indicated for peribiliary cysts, but the cysts can multiply and increase in size over time [7]. This can lead to bile duct obstruction, which may have functional significance could cause clinical symptoms if left untreated [3]. Serum CA 19-9 elevation is reported in some cases, but is considered more likely related to bile duct obstruction and associated inflammation rather than to peribiliary cysts themselves [3,9]. Symptomatic patients should undergo an MRCP or ERCP and can be diagnosed with surgical resection or fine needle aspiration [13].
In our patient, stricture and dilatation of the left hepatic bile duct were monitored regularly. When she became symptomatic for the first time, she had a low-level hyperbilirubinemia (27 μmol/l) and significantly elevated serum CA 19-9 (640 U/ml), likely due to diagnosed cholecystitis, cholecystolithiasis and cholangiosepsis. During the subsequent episodes of cholangiosepsis, serum bilirubin was significantly elevated (125.7 μmol/l), suitable to advanced bile duct compression.
Peribiliary cysts are a poorly recognised disease in clinical practice and misdiagnosis with consecutive false treatment has been reported [19,20]. Common incorrect diagnosis include Caroli’s disease or intrahepatic cholangiocarcinoma [8,16,21,22]. A systematic review revealed an misdiagnosis by imaging modalities in 38% of cases and therapeutic mistreatments in 36% of Type I and III peribiliary cysts [2].
In our patient, although Nakanuma cysts were diagnosed after surgical procedure only, the treatment was appropriate. Observation of the known stricture and poststenotic dilatation of the left bile duct was performed after negative cytology in ERCP as long as the patient stayed asymptomatic. Surgical intervention became necessary after ten years due to recurrent cholangiosepsis.
This case report aims to raise awareness of peribiliary cysts in clinical practice. They should be considered as a potential cause of bile duct obstruction and kept in mind as a differential diagnosis to Caroli’s disease and cholangiocarcinoma on imaging. Correct diagnostic is crucial to avoid misdiagnosis and subsequent overtreatment.
Abbreviations: ADPKD: Autosomal Dominant Polycystic Kidney Disease; ADPLD: Autosomal Dominant Polycystic Liver Disease; AIH: Autoimmune Hepatitis; CA 19-9: Carbohydrate Antigen 19-9; CECT: Contrast-Enhanced Computer Tomography; CT: Computer Tomography; DIC-CT: Drip Infusion Cholangiographic Computer Tomography; ERCP: Endoscopic Retrograde Cholangiopancreatography; IPMN: Intraductal Papillary Mucinous Neoplasm; MRCP: Magnetic Resonance Cholangiopancreatography; MRI: Magnetic Resonance Imaging; PBC: Primary Biliary Cholangitis; PKD1: Polycystic Kidney Disease Gene 1; PKD2: Polycystic Kidney Disease Gene 2; SLE: Systemic Lupus Erythematosus; Sjs: Secondary Sjögren’s Syndrome.
Conflict of interest: The authors have no conflict of interest to disclose.
Data availability: All patient data related to this case report is available on request.
Ethical statement: The patient provided informed consent for the presentation of the case and visual material.
References
- Nakanuma Y, Kurumaya H, Ohta G. Multiple cysts in the hepatic hilum and their pathogenesis. A suggestion of periductal gland origin. Virchows Archiv. A, Pathological anatomy and histopathology. 1984; 404.
- Bazerbachi F, Haffar S, Sugihara T, et al. Peribiliary cysts: A systematic review and proposal of a classification framework. BMJ Open Gastroenterol. 2018; 5.
- Pang T, Kuo S, Hugh TJ, et al. The role of peribiliary cysts in biliary obstruction. ANZ journal of surgery. 2010; 80.
- Terada T, Nakanuma Y. Pathological observations of intrahepatic peribiliary glands in 1,000 consecutive autopsy livers. III. Survey of necroinflammation and cystic dilatation. Hepatology. 1990; 12: 1229-33.
- Okada S, Kojima Y, Morozumi A, Ainota T, Miyazaki Y, et al. Multiple hepatic peribiliary cysts discovered incidentally at a medical examination. Journal of gastroenterology and hepatology. 2001; 16: 1167-9.
- Miura F, Takada T, Amano H, et al. A case of peribiliary cysts accompanying bile duct carcinoma. World J Gastroenterol. 2006; 12: 4596-8.
- Uski ACVR, Pedroso MHNI, Abud CP, Costa MM, Ferreira MPFD. Peribiliary cysts: uncommon mimickers of hepatic and biliary cystic lesions. Abdom Radiol (NY). 2024.
- Kim HJ, Kim CY, Hur YH, Kim JC, Cho CK, Kim HJ. Peribiliary cysts developed in normal underlying liver: report of a case. Korean J Hepatobiliary Pancreat Surg. 2013; 17: 131-4.
- Wongwattanachai A, Luvira V, Pairojkul C. Peribiliary Cyst: An Unusual Mimicker of Cystic Liver Lesions. GE Port J Gastroenterol. 2023; 30: 322-6.
- Nakanuma Y. Peribiliary cysts have at least two different pathogeneses. J Gastroenterol. 2004; 39: 407-8.
- Matsubara T, Kozaka K, Matsui O, et al. Peribiliary glands: Development, dysfunction, related conditions and imaging findings. Abdom Radiol (NY). 2020; 45: 416-36.
- Seguchi T, Akiyama Y, Itoh H, et al. Multiple hepatic peribiliary cysts with cirrhosis. J Gastroenterol. 2004; 39: 384-90.
- Yu-Xiang Ye, Tobias Hepp, Michael Bitzer, Marius Horger. Peribiliäre Zysten. Rofo. 2020; 192: 7-11.
- Ohira H, Abe K, Takahashi A. Involvement of the liver in rheumatic diseases. Clin J Gastroenterol. 2012; 5: 9-14.
- Ikenaga N, Chijiiwa K, Otani K, Ohuchida J, Uchiyama S. A case of peribiliary cyst presenting with obstructive jaundice. J Gastrointest Surg. 2009; 13: 174-6.
- Su W-L, Chang W-T, Wang S-N, Chuang S-C, Kuo K-K, et al. Solitary peribiliary cyst mimicking cholangiocarcinoma. Formosan Journal of Surgery. 2013; 46: 61-4.
- Yokomichi H, Tsuji K, Hayashi Y, et al. A case of multiple hepatic peribiliary cysts which contributed to the obstructive jaundice and led to liver failure at the young man with von Recklinghausen’s disease. Hepatol Res. 2006; 35: 222-7.
- Baron RL, Campbell WL, Dodd GD. Peribiliary cysts associated with severe liver disease: imaging-pathologic correlation. AJR Am J Roentgenol. 1994; 162.
- Narayan RR, Juakiem WY, Poultsides GA, El-Dika S. Peribiliary cysts masquerading as choledocholithiasis. Video GIE. 2023; 8: 351-3.
- Nakanuma Y. Peribiliary cysts: A hitherto poorly recognized disease. Journal of gastroenterology and hepatology. 2001; 16: 1081-3.
- Stevens W, Harford W, Lee E. Obstructive jaundice due to multiple hepatic peribiliary cysts. Am J Gastroenterol. 1996; 91: 155-7.
- AlNuaimi D, Balci NC, AlDuaij A, AlKetbi R, Sierra MPR. A case of peribiliary hepatic cysts in a cirrhotic liver: A mimicker of Klatskin Tumor. Radiol Case Rep. 2020; 15: 1039-43.
