
Open Access, Volume 10
Actinobacillus hepaticus with cryptococcal infection: Case report
Yiming Zhang1; Changfa Cheng1; Yanan Zhai1,2; Shunlin Guo1,2*
1Department of Radiology, The First Clinical Medical College of Lanzhou University, Lanzhou, 730000, China.
2Department of Radiology, The First Hospital of Lanzhou University, Lanzhou, 730000, China.
Shunlin Guo
Department of Radiology, The First Hospital of Lanzhou University, Lanzhou, 730000, China.
Email: guoshl@lzu.edu.cn
Received : June 29, 2024,
Accepted : July 20, 2024
Published : July 30, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Co-infection with Actinobacillus hepaticus and Cryptococcus is a rare and complex condition frequently observed in individuals with compromised immune systems. The clinical and imaging manifestations of this condition are nonspecific, rendering it highly susceptible to misdiagnosis and necessitating reliance on pathology for a definitive diagnosis. This case describes a patient co-infected with Actinobacillus and Cryptococcus. Neoplastic lesions and bacterial infections were ruled out based on imaging findings, leading to a focus on fungal infections. This case provides a valuable reference for future studies, highlighting the need to further investigate co-infection mechanisms and optimize treatment strategies.
Keywords: Hepatic infections; Actinobacillus; Cryptococcal; Magnetic resonance imaging.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Giordano A et al
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Zhang Y, Cheng C, Zhai Y, Guo S. Actinobacillus hepaticus with cryptococcal infection: Case report. Open J Clin Med Case Rep. 2023; 2266.
Clinical Information
A 56-year-old male patient was admitted to the hospital due to persistent fatigue and shortness of breath lasting for more than 2 months. An ultrasound (Figure 1) performed at an external facility revealed a hepatic shadow that has not improved despite treatment. On April 12, 2017, the patient underwent pancreaticoduodenectomy followed by intraperitoneal chemical particle implantation for the treatment of a pancreatic cyst associated with chronic pancreatitis. Laboratory tests revealed elevated levels of C-reactive protein and abnormal liver function. AFP (-), CEA (-). MRI of the abdomen (Figure 2A-G) showed a large mass measuring approximately 81×61 mm in the right posterior lobe of the liver, characterized by a “double-ring” appearance at the edge. The mass exhibited low signal intensity on T1WI, slightly high signal on T2WI, mild diffusion restriction on DWI, inhomogeneous enhancement on the arterial phase, decreased enhancement in both the venous and delayed phases, and low uptake on the hepatobiliary phase. Localized intrahepatic bile duct invasion within the right lobe of the liver, accompanied by distal dilatation, edema, and abnormal perfusion of the surrounding liver tissue. MRI findings suggest a possible infectious liver lesion, and the tumor could not be drained. Pathological sections of the biopsy obtained from the local hospital consultation (Figure 3) showed fibrous tissue hyperplasia, foam-like histiocyte aggregates observed under the microscope, small spherical fungi with a powder-stained appearance in the cytoplasm, significant neutrophilic infiltration in the interstitium, and filamentous mycobacterial clusters visible at the tissue edge. Rabbit immunohistochemistry of tissue block B showed positive staining for CK (Pan) in residual hepatocytes and for CD68 in histiocytes. Special stains performed on tissue block B revealed reticular scaffold breaks on Masson staining, reticular fibers, positive staining with PAS, and silver stains. The pathological diagnosis of the liver tissue demonstrated morphology consistent with Actinomyces infection, with special staining suggesting a concomitant Cryptococcal infection.
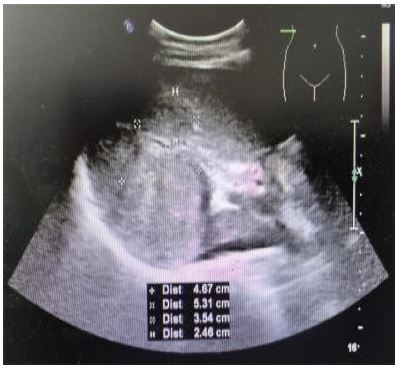
Figure 1: Image of ultrasound revealed a hepatic shadow.
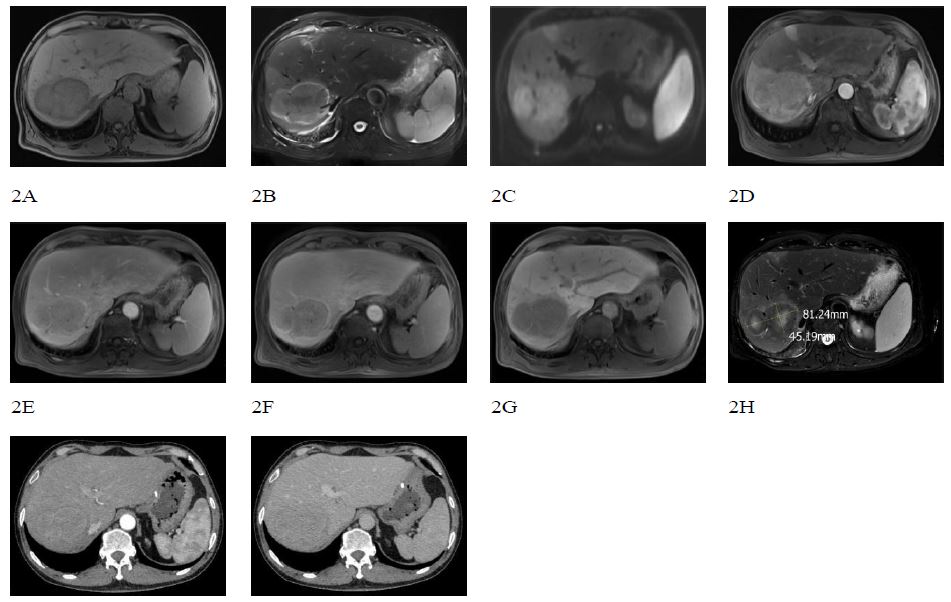
Figure 2A-G: Image of Actinobacillus hepaticus with Cryptococcal infection.
A. TIWI B. T2WI C. DWI D. MRI enhanced arterial phase E. MRI enhanced venous and delayed phase F. MRI enhanced delayed phase G. hepatobiliary phase H. Post-treatment T2WI
A. TIWI B. T2WI C. DWI D. MRI enhanced arterial phase E. MRI enhanced venous and delayed phase F. MRI enhanced delayed phase G. hepatobiliary phase H. Post-treatment T2WI
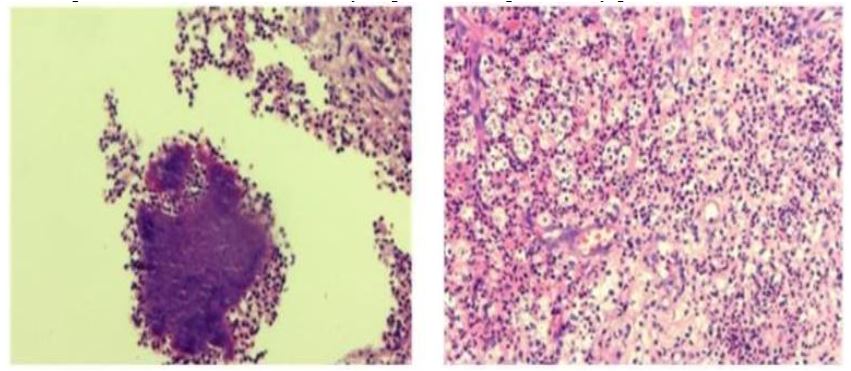
Figure 3: Image of Actinobacillus hepaticus with cryptococcal infection.
The left image is Actinobacillus hepaticus by hematoxylin-eosin staining (×200)
The right imge is Cryptococcus hepaticus by periodic acid- schiff and periodic-acid silver methenamine staining (×200)
Disscussion
Actinomycosis is an uncommon, chronic suppurative inflammatory and granulomatous lesion primarily caused by actinomycete infection [1]. The condition was first described by pathologist Otto Bollinger in 1877, who noted sinusoidal tract formation and expulsion of sulfur particles as its main features [2]. They are commensal in the human oral cavity, gastrointestinal tract, and pelvic mucosa [3]. Actinomycosis has various subtypes depending on the site of involvement, including cervicofacial (50%), thoracic (15%), and abdominopelvic (20%), which are the most common types reported [4]. Hepatic actinomycosis is exceptionally rare, accounting for only 5% of reported cases [5]. Actinomycetes, being opportunistic pathogens, are more likely to cause infection in individuals with susceptibility factors such as diabetes mellitus, immunosuppression, malnutrition, prior surgery, oral tumours or infections, and radiotherapy for head and neck malignancies [6]. Abdominopelvic actinomycosis manifests with nonspecific clinical features, mainly presenting as persistent lower abdominal pain and the presence of an abdominal mass. This case is categorized as abdominopelvic type, with clinical and imaging manifestations that are nonspecific. Consequently, it is prone to misdiagnosis as either inflammation or a tumor [7].
Cryptococcosis is an infection caused by pathogenic, encapsulated yeasts of the genus Cryptococcus. Approximately 95% of cryptococcal infections are attributed to novel strains of Cryptococcus, specifically serotype A [8]. This opportunistic pathogen is commonly found in pigeon droppings and soil and can cause cryptococcosis. The infection primarily affects immunocompromised individuals, including those with acquired immunodeficiency syndrome, undergoing immunosuppressive therapy, corticosteroid therapy, or malignancy. Meningitis and pneumonia are common clinical manifestations in patients with cryptococcosis. Although the liver is not a common site for primary cryptococcal infections, hepatobiliary cryptococcosis has been reported as a manifestation of either disseminated or isolated cryptococcosis in immunocompromised individuals [9].
The patient did not present with manifestations of meningitis or pneumonia, and his immunological markers were within normal ranges, which is inconsistent with existing literature. The patient exhibited abnormal liver function and imaging findings consistent with early cirrhosis and had previously undergone pancreaticoduodenectomy, which is speculated to be associated with this bacterial infection. However, co-infection with Actinobacillus and Cryptococcus is rare; thus, further investigation into its pathogenesis is warranted. This case represents a fungal liver infection and needs to be differentiated from liver abscess and hepatocellular carcinoma.
1. Differentiation from liver abscess: (1) In this case, there was no stratification within the lesion, and multiple small spots presented as the "pretzel sign," a characteristic feature that may serve as a clue to the diagnosis of fungal infection. (2) Additionally, the diffusion restriction observed in DWI was mild.
2. Differentiation from hepatocellular carcinoma (HCC): This case exhibits "fast in and fast out" enhancement on MRI; however, the enhancement changes are not apparent on CT, which is inconsistent with typical hepatocellular carcinoma. The "fast-in-fast-out" MR enhancement may be attributed to the background enhancement of the liver parenchyma following the injection of a specific contrast agent, leading to pseudo-enhancement of the lesion.
3. Medical Treatment: The recommended treatment regimen for actinomycosis involves a high dose and complete course of penicillin [4]. In this case, the initial anti-infective therapy included doxycycline and amphotericin B administered at the appropriate total dose and duration. Subsequently, the antibiotic regimen was modified, and the patient was administered fluconazole for over one week. Upon review of the liver MRI, the lesion size was reduced compared to the image taken one week earlier (Figure 2H), and the edema of the peripheral liver parenchyma was also diminished, accompanied by new necrosis in the center of the lesion. This observation indicates that the antibiotic treatment was effective and supports the pathological diagnosis.
References
- MA Lin, LU Qiang, LING Wenwu, et al. A case of hepatic actinomycosis misdiagnosed as hepatocellular carcinoma [J]. China Medical Imaging Technology. 2013; 29(04): 671-672. DOI:10.13929/j.1003-3289.2013.04.024.
- Madison B, Jack A, Ishad A. The diagnosis and management of pulmonary actinomycosis [J]. Journal of Infection and Public Health. 2023; 16(4): 490-500.
- Siregar GRD, Kawilarang PA, Kusumaningrum D, et al. A rare case report of liver masses caused by Actinomyces species [J]. Indian journal of medical microbiology. 2024; 49100573-100573.
- LI Chenxia, ZHANG Jianxin. Clinical misdiagnosis and literature review of pelvic and abdominal actinomycosis invading multiple organs [J]. Clinical Misdiagnosis and Mistreatment. 2017; 30(04): 10-13.
- M MM, Anastasia N, Nirali S, et al. S3756 Hepatic Actinomycosis: A Rare Culprit in Liver Infections [J]. The American Journal of Gastroenterology. 2023; 118(10S): S2422-S2423.
- LI Xiuli, LI Xiangcui, LIAO Wan. Research progress of actinomycosis, Chinese Journal of Mycology. 2008; 3(3): 189-192.
- YANG Jing, LIU Xiaoqing, DANG Guohua. Clinical Characteristics and Treatment of Actinomycosis, Chinese Family Medicine. 2009; 12(7A): 1206-1208.
- Maziarz EK, Perfect JR. Cryptococcosis. Infect Dis Clin North Am. 2016; 30(1): 179-206. doi:10.1016/j.idc.2015.10.006. PMID:26897067; PMCID: PMC5808417.
- Zhu M, Wang Q, Wang M, et al. Rare Hepatic Cryptococcosis Mimicked Metastatic Liver Cancer and Confirmed by Metagenomic Next-Generation Sequencing in an Immunocompetent Patient: A Case Report. Infect Drug Resist. 2022; 15: 5753-5758https://doi.org/10.2147/IDR.S381730.
