
Open Access, Volume 10
Erythema multiforme - A classic presentation
Chaithra KM*; Kruthika S Guttal; Venkatesh Naikmasur; Kirty R Nandimath
Department of Oral Medicine & Radiology, SDM College of Dental Sciences & Hospital, Shri Dharmasthala Manjunatheshwara University, Sattur, Dharwad -580009, India.
Chaithra KM
Department of Oral Medicine and Radiology, SDM College of Dental Sciences & Hospital, Shri Dharmasthala Manjunatheshwara University Sattur, Dharwad-580009, India.
Tel: 9846629666;
Email: chaithrakm666@gmail.com
Received : June 26, 2024,
Accepted : July 15, 2024
Published : July 30, 2024,
Archived : www.jclinmedcasereports.com
Keywords: gastrointestinal metastases; invasive lobular breast carcinoma; pathohistological analysis; immunohistochemical analysis; complex treatment.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Chaithra KM (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Chaithra KM, Guttal KS, Naikmasur V, Nandimath KR. Erythema multiforme - A classic presentation. Open J Clin Med Case Rep. 2024; 2265.
Description
A 48-year-old male presented with rapid onset of ulcerations on the lower lip, progressively spreading to the buccal mucosa, tongue, and upper lip, associated with burning sensation and difficulty in eating and drinking. A prodrome of fever (one week prior), preceded the ulcerations on the lowerlip & skin lesions on the hands and legs. Patient was under treatment for hypothyroidism & hypertension. Examination revealed a classic “target” or “bull’s-eye” lesion of central necrosis with concentric rings on the palms (Figure 2a) and legs (Figure 2b), and diffuse ulceration all over the upper and lower lip (Figure 2a) , buccal mucosa (Figure 2b), palate, dorsal surface of tongue on the left side, ventral surface of the tongue, labial mucosa and lips with erythema surrounding with irregular margin. The lesion over the vermillion border was showing mild crustation covered with yellowish slough which was bleeding on examination and was velvety in consistency and tender on palpation. Marked halitosis was noted during examination. Based on history and presentation a diagnosis of Erythema Multiforme (EM) was made. EM is a widespread hypersensitivity reaction that manifests with varying degrees of severity. The characteristic target lesion in Erythema multiforme is one of the primary diagnostic criteria for the disease.
The therapy regimen included a broad-spectrum antibiotic Tab.Azithromycin 500 mg to tackle potential bacterial infections, Tab. Aceclofenac (100 mg) + Paracetamol (325 mg) for pain relief, Tab. Deflazacort (6 mg t.i.d) for 5 days (tapering done). Concurrently, Multivitamin supplement was given with an addition of antacid. Oral hygiene is maintained with Povidone Iodine (2% w/v) and Benzydamine mouthwash (0.15% w/v), alongside local treatment using Triamcinolone Oromucosal paste (0.1% w/w). Dermatological symptoms are managed with Fluticasone propionate (0.05%w/w), and additional nutritional support is provided through Protein supplement. This comprehensive approach ensures that the patient’s symptoms are addressed systematically while supporting their overall well-being and recovery.
Keymessage: The diagnosis of Erythema Multiforme primarily relies on the history of lesion eruption and associated clinical findings, which are crucial indicators. Typically, the clinical course of EM is self-limiting, with symptoms resolving within weeks; however, severe cases may necessitate hospitalization for hydration, analgesia, antiviral therapy, and systemic steroids. Equally vital is providing supportive care, managing infections, and discontinuing precipitating agents to ensure optimal management and recovery.
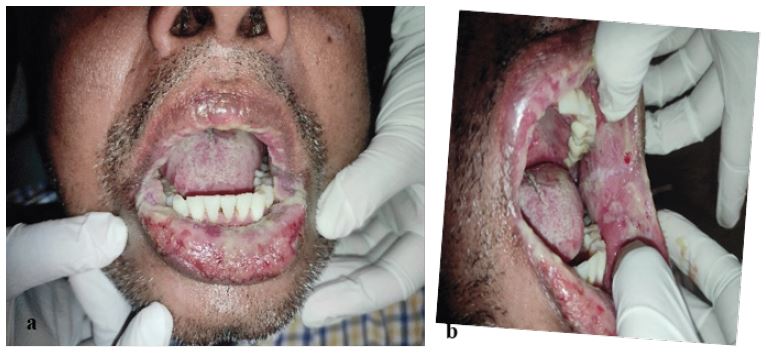
Figure 1: Diffuse ulceration on the lower lip (a) and left buccal mucosa overlying pseudomembranous slough (b).

Figure 2: Classic target lesion of central necrosis with concentric rings on the palms(a) and legs(b).

Figure 3: Follow up after two weeks showing regression of lesions.
