
Open Access, Volume 10
Atypical febrile illness caused by an emerging opportunistic pathogen Roseomonas gilardii: A case report
Niti Bhai1; Chand Nigam1; Anjali Tewari2; Devendra Niranjan1; Pradeep Paul1*; Arvind Singh3; Rashmi Kapoor3
1Department of Microbiology, Regency Hospital Ltd, Kanpur, India.
2Department of Pathology, Regency Hospital Ltd, Kanpur, India.
3Department of Pediatrics, Regency Hospital Ltd, Kanpur, India.
Pradeep Paul
Department of Microbiology, Regency Hospital, A2, Sarvodaya Nagar, Kanpur, India.
Email: pradeep.gacc@gmail.com
Received : June 15, 2024,
Accepted : July 09, 2024
Published : July 10, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Roseomonas gilardii is a rare pathogen which has been reported to cause bacteremia and other systemic infection in a chronic debilitated patient. Here in this report we discuss a case of 3 yr old, male, patient who presented with symptoms of acute onset fever with multiple episodes of seizures and postictal drowsiness. The patient was admitted in the PICU and managed conservatively with i.v midazolam, ceftriaxone, sodium valproate and paracetamol. On the next day patient became afebrile, conscious with no further episodes of seizures. EEG and chest X-ray was normal, urine R/M was inconclusive and among biochemical parameters serum sodium level was slightly low. Single blood culture from the peripheral catheter shows slimy, mucoid growth of gram negative bacteria on blood agar which was identified as Roseomonas gilardii by Vitek-2 system after 6 days of incubation which was sensitive to cephalosporins, carbapenems and aminoglycosides. Patient was discharged after 3 days of treatment with follow up advice. Physicians should be aware of themselves with the characteristics of infection with R. gilardii because of diagnostic challenges and patient management. This organism should be considered in the differential diagnosis when a patient present with underlying debility and sepsis in the presence of a central or peripheral line, especially if there is no other focus of infection and no growth on blood culture for 3 to 4 days.
Keywords: Bacteremia; Seizures; Mucoid; Gram negative; Central line; Peripheral.
Abbreviations: PICU: Pediatric Intensive Care Unit; EEG: Electroencephalogram; R/M: Routine Microscopy.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Paul P (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Bhai N, Nigam C, Tewari A, Niranjan D, Paul P, Singh R, Kapoor R. Atypical febrile illness caused by an emerging opportunistic pathogen Roseomonas gilardii: A case report. Open J Clin Med Case Rep. 2024; 2264.
Introduction
Roseomonas gilardii is an emerging opportunistic pathogen that has been indicated as a rare cause of human infections. Roseomonas genus was described in 1993 by Rihs et al. as a ‘‘pink coccoid’’, non-fermentative, aerobic, gram negative bacteria. It has been isolated from environmental sources (e.g., water, soil, air, and plants). The population structure of the genus showed clades associated with humans, whereas others grouped environmental strains only. Roseomonas gilardii and Roseomonas mucosa are the species known to infect human and the opportunistic infections due to them are related to the patient skin microbiota rather than to the environment [1]. More data would be needed to understand the reservoirs of these opportunistic pathogens that have long been considered as of environmental origin. Their cultural characteristics as well as the antimicrobial sensitivity pattern would be helpful to improve infection control practices, make accurate diagnosis and for better patient management.
Case Report
A 3 yr old male child presented to the pediatrician with a one day history of chills, fever to upto 101°F with multiple episodes of seizures and post-ictal drowsiness. On examination, body weight was 15 kg, heart rate was 128/min, respiratory rate- 28/min, peripheral pulse was present, volume normal, bilateral chest A/E, P/A soft, CVS S1 S2 normal, CNS tone normal. Based on the history and examination the patient was admitted to PICU for the prompt management. Immediate investigations like EEG, Chest X-ray, biochemical parameters, blood culture and urine R/M was ordered and the patient was conservatively managed with i.v fluids, oxygenation through mask, midazolam 2 ml in 10 ml normal saline over 10 hours, ceftriaxone 750 mg i.v 12 hourly, paracetamol 23 ml 6 hourly along with loading dose of sodium valproate 300 mg in 10 ml normal saline followed by 150 mg i.v 12 hourly. On the next day the patient became afebrile and vitals where within normal limits with no further episodes of seizures seen. CNS evaluation was done and the child was found active, conscious and well-oriented. The child was allowed to take oral food, oxygen therapy was stopped and mannitol 30 ml i.v was added to the treatment regime. EEG and chest X-ray was normal, urine R/M was inconclusive and among biochemical parameters serum sodium level was 134.2 (biological ref. range 138-148 mEq/L). Only single blood culture bottle was sent to the microbiology lab from peripheral catheter on the day of admission. The blood culture bottle was immediately put into BacTalert automated blood culture system which flagged positive after 6 days of incubation. The positive blood culture bottle was subcultured on Blood agar and MacConkey agar and simultaneously a gram stain was prepared directly from the positive blood culture bottle which showed gram negative bacilli with which was telephonically reported to the treating consultant as a critical alert. After overnight incubation there were dull white, slimy, mucoid, runny bacterial colonies were seen on blood agar plate and no growth was seen on MacConkey agar after extended incubation for 72 hrs. Few isolated bacterial colonies were picked up and automated antimicrobial sensitivity was performed using Vitek-2 system which identified it as Roseomonas gilardii but failed to provide the antimicrobial sensitivity due to lack of data for this rare organism. So Kirby-Bauer disc diffusion method was used for the antimicrobial susceptibility testing. The organism was susceptible to Ceftriaxone, Piperacillin-Tazobactam, Cefoperazone-Sulbactam, Cefepime, Imipenem, Meropenem, Tetracycline, Doxycycline, Minocycline, Gentamicin, Amikacin, Tobramycin and resistant to Ampicillin-Sulbactam, Ceftazidime, Ciprofloxacin and Cotrimoxazole. A second blood culture was also sent after 3 days of the treatment which showed no growth after 7 days of incubation. On the 3rd day of admission the child was again evaluated and was found afebrile, well active and conscious and as the EEG and MRI reports were inconclusive with no further episodes of seizures, the patient was discharged home on day 3, continued on home syrup valproic acid (200/5) 3.5 ml twice a day and syrup calcium 2.5 ml twice a day for 1 month and follow up after 7 days.
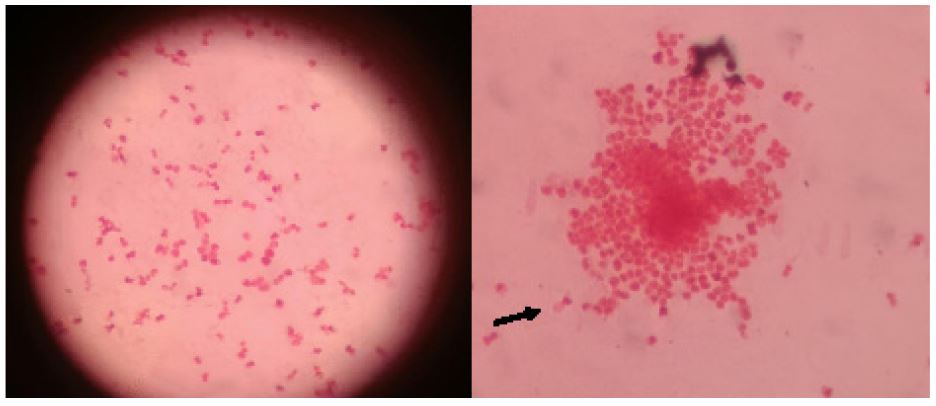
Figure 1: Roseomonas gilardii on Gram stain from culture plate (Pink, coccoid, vacuolated cells).
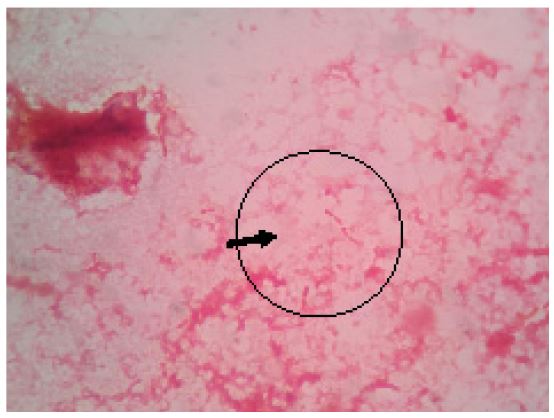
Figure 2: Bacillary form of Roseomonas gilardii on Gram stain of direct blood culture bottle.
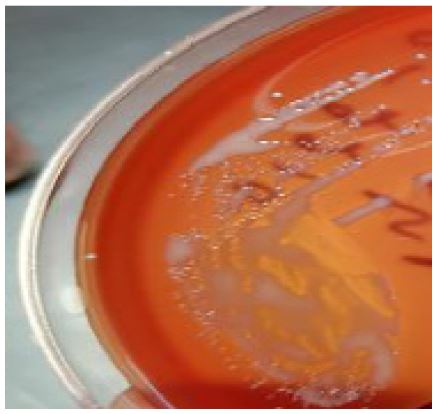
Figure 3: Mucoid, runny colonies of Roseomonas gilardii on blood agar.
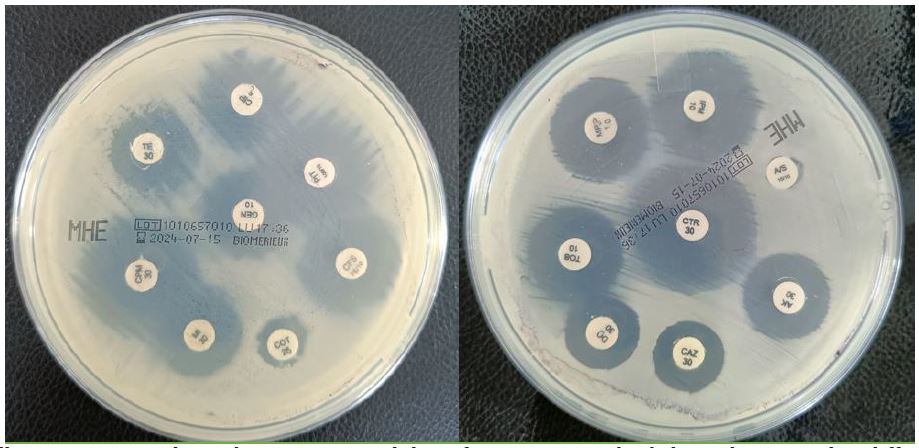
Figure 4: Mueller Hinton Agar plates showing susceptibility of Roseomonas gilardii by Kirby Bauer disc diffusion method.
Discussion
At present, about 40 case reports described clinical infections caused by Roseomonas spp., providing complete overview about vulnerabilities to infection, clinical presentations and treatments [1-4]. Infections in humans have mainly been documented during primary or healthcare-associated infections in patients with underlying diseases and/or indwelling devices [1-4]. Our case demonstrates some features in common with case reports and case series of patients found to have infections with R. gilardii. The natural reservoir for this infection is unknown. It may exist as a commensal in humans and it has also been isolated from water supplies [5-8]. Out of number of the cases of R. gilardii infections reported in the literature (14 of 25 [56%]), showed the initial symptoms of infection and bacteremia. This outcome is often associated with the presence of a central line (9 of 25 cases reporting clinical information) based on the case reports till now [7-9]. Other sites of infection have also been reported; respiratory problems occurred in 16% of cases, wound infection or bone disease occurred in 8%, peritonitis in 4%, enteritis and/or abdominal pain in 8%, kidney transplant infection in 4%, and eye infection in 4% [7-9]. A typical feature of this organism is its slow-growth properties on culture as it often takes 4 to 5 days to grow. Most of the report analysis reveals that in 88% of these cases, the organism was isolated from the blood [7-9]. Often it was isolated from only one of several blood cultures or from a central venous catheter line and not the peripheral blood sample unlike our case report in which it was isolated from the peripheral line. Regarding antibiotic susceptibility pattern, this organism shows variability in sensitivity especially with regard to its behavior with cephalosporins, which appear ineffective against any of the Roseomonas species. Rihs found that all six species exhibited 96% resistance to cephalosporins including expanded-spectrum generation cephalosporins: cefotaxime, ceftriaxone, and ceftazidime. In contrast, Lewis reports that all of her isolates were susceptible to cefotaxime [9], with at least two of her patients making a complete recovery on cefotaxime which is in concordance with our caase report. Susceptibility to “fourth-generation” cephalosporins, such as cefepime and cefpirome is still under evaluation [10]. The species has universal susceptibility to imipenem, amikacin, gentamicin, tobramycin, and tetracycline. It is largely resistant to penicillins, including the extended-spectrum penicillins such as piperacillin and mezlocillin. Addition of a beta-lactam can increase susceptibility. Despite the fact that this Roseomonas gilardii infection seems to occur in immunocompromised or debilitated patients, reported mortality due to it is relatively low and patients do usually recover completely. We believe that R. gilardii was the causative organism in our case described here due to several reasons. First, the patient’s systemic symptoms were at their height on the day that the positive blood culture was drawn and it grew from single aerobic blood culture bottle. Although only one blood culture became positive, this is consistent with other cases reported in the literature, all of which report that only one of several blood cultures grew the organism. In our case 2nd blood culture which was sent on the day of discharge was negative which may be due to the effect of antibiotic ceftriaxone which might have made the blood sterile. Bacterial growth also took 6 days, which was consistent with the slow-growth properties reported elsewhere. The clinical presentation that we observed is also almost identical to that of other cases: namely, presentation with systemic symptoms of infection with bacteremia. Unlike other patients, this patient did not have any underlying debility and nor any central line was in place. Although the probable source of infection in this case could be the skin, we were not able to isolate the infecting organism from there. However, this is also consistent with previous findings, in that only one case has been reported in which this organism has been successfully cultured from the skin. As in the majority of other cases, our patient made a complete recovery with treatment. Physicians should be aware with the characteristics of infection with R. gilardii to overcome diagnostic challenges and for better patient management. This organism should be considered in the differential diagnosis when a patient present with underlying debility and sepsis in the presence of a central line, especially if there is no other focus of infection and no growth on blood culture for 3 to 4 days. In addition, contamination should not be immediately assumed if only one blood culture is positive. It is important to pursue final identification of the organism for accurate susceptibilities to antibiotics. Consideration of gram-negative coverage with an aminoglycoside rather than a cephalosporin would be reasonable.
Acknowledgements: I would like to pay my sincere gratitude to our Director of laboratory sciences Dr. Anjali Tewari for her guidance and support. Also I would like to thank Regency Health for providing us the advanced diagnostic facilities.
References
- Shokar NK, Shokar GS, Islam J, Cass AR. Roseomonas gilardii infection: Case report and review. J Clin Microbiol. 2002; 40: 4789e91.
- De I, Rolston KVI, Han XY. Clinical significance of Roseomonas species isolated from catheter and blood samples: analysis of 36 cases in patients with cancer. Clin Infect Dis. 2004; 38: 1579e84.
- Sipsas NV, Papaparaskevas J, Stefanou I, Kalatzis K, Vlachoyiannopoulos P, et al. Septic arthritis due to Roseomonas mucosa in a rheumatoid arthritis patient receiving infliximab therapy. Diagn Microbiol Infect Dis. 2006; 55: 343e5.
- Wang CM, Lai CC, Tan CK, Huang YC, Chung KP, et al. Clinical characteristics of infections caused by Roseomonas species and antimicrobial susceptibilities of the isolates. Diagn Microbiol Infect Dis. 2012; 72: 199e203.
- Michon AL, Saumet L, Bourdier A, Haouy S, Sirvent N, et al. Bacteremia due to imipenem-resistant Roseomonas mucosa in a child with acute lymphoblastic leukemia. J Pediatr Hematol Oncol. 2014; 36: e165e8.
- Rihs JD, Brenner DJ, Weaver RE, Steigerwalt AG, Hollis DG, et al. Roseomonas, a new genus associated with bacteremia and other human infections. J. Clin. Microbiol. 1983; 31: 3275-3283.
- Sandoe JAT, H Malnick, KW Loudon. A case of peritonitis caused by Roseomonas gilardii in a patient undergoing continuous ambulatory peritoneal dialysis. J. Clin. Microbiol. 1997; 35: 2150-2152.
- Struthers M, J Wong, JM Janda. An initial appraisal of the clinical significance of Roseomonas species associated with human infections. Clin. Infect. Dis. 1996; 23: 729-733
- Lewis L, SF Stock, D Williams, S Weir, VJ Gill. Infections with Roseomonas gilardii and review of characteristics used for biochemical identification and molecular typing. Am. J. Clin. Pathol. 1997; 108: 210-216.
- Nahass RG, R Wineski, DJ Herman, E Hirsh, K Goldblatt. Vertebral osteomyelitis due to Roseomonas species: Case report and review of the evaluation of vertebral osteomyelitis. Clin. Infect. Dis. 1995; 21: 1474-1476.
- Lewis L, SF Stock, D Williams, S Weir, VJ Gill. Infections with Roseomonas gilardii and review of characteristics used for biochemical identification and molecular typing. Am. J. Clin. Pathol. 1997; 108: 210-216.
