
Open Access, Volume 10
Successful caesarean myomectomy in primigravidae: Case series
John Deogratias Tilubuzya Lawi1*; Alfred Mwakalebela Laison1; Scholastica Mathew Malangalila1; Francis Richard Kwetukia1; Patrick Kushoka2; Godbless Kimaro Nelson2
1Department of Obstetrics and Gynecology, Iringa Regional Referral Hospital, Tanzania.
2Department of Obstetrics and Gynecology, University of Dodoma, Tanzania.
John Deogratias Tilubuzya Lawi
Department of Obstetrics and Gynecology, Iringa Regional Referral Hospital, Tanzania.
Email: lawi.john@yahoo.com
Received : June 11, 2024,
Accepted : July 04, 2024
Published : July 10, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Even though myomectomy during caesarean section is usually avoided due to the risks of bleeding and postoperative complications, it can be done successfully with careful patient selection and, in some cases, in an emergency, with the presence of a competent surgeon and access to blood transfusion facilities. This was proved by two cases of primigravidae women who underwent an emergency and an elective caesarean myomectomy. The bleeding was successfully controlled by two-layer closure of the caesarean and myomectomy incisions and the administration of oxytocin misoprostol, tranexamic acid and application of uterine compression sutures resulting in a positive outcome for both mothers and babies, who were discharged on day four and seven after surgery respectively.
Keywords: Caesarean myomectomy; Primigravida; Myoma; Caesarean section; Pregnancy
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Lawi John DT (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Lawi John DT, Laison AM, Malangalila SM, Kwetukia FR, Kushoka P, Nelson GK. Successful caesarean myomectomy in primigravidae: Case series. Open J Clin Med Case Rep. 2024; 2262.
Introduction
Uterine myomas are common during pregnancy, affecting up to 11.2% of women [1,2]. It is also prevalent in elderly primigravidae [3,4]. Uterine myomas most commonly occur in the fundus and upper uterine region, accounting for around 80% of cases [5]. Although myomectomy during pregnancy is unusual, it can be performed safely in carefully selected cases with little risk of severe bleeding or complications [6,4]. These case series demonstrate the safety and practicability of performing emergency and elective caesarean myomectomies in primigravidae women in low-resource settings.
Case Series
Case 1: A 38-year-old first-time pregnant woman was hospitalised in the prenatal ward at a gestational age of 39 weeks. She reported three days of lower abdomen pain with no vaginal bleeding or discharge and regular bowel movements. Her uterus measured 40 cm by Symphysis Fundal Height estimation; she had three uterine contractions in 10 minutes lasting for 30 seconds; the foetal heart rates were 136 in a minute; and she had cervical dilation of 5 centimetres. An obstetric ultrasound was done and revealed a single living foetus with a cephalic presentation, an estimated weight of 2389 gm, and a gestational age of 39 weeks. The placenta was found in the anterior fundal, with grade 2 placental calcification and a myoma on the lower part of the uterus that was blocking the internal cervical canal. The patient had four prenatal checkups and was not HIV, Syphilis, or Malaria positive. Despite undergoing hematinics, deworming, and Intermittent Preventive Treatment for Malaria, she was anaemic, with a haemoglobin estimate of 10.6 g/dl. She had never had any ultrasound done before during all the antental visits, and there was no clinical diagnosis for uterine myoma in pregnancy.
Due to the myoma’s position, which offered a risk of impeding delivery, the patient underwent emergency caesarean surgery on 5th October 2021. Before the surgery, the anaesthetist reviewed the patient’s condition. Her haemoglobin level was 13.3 g/dl, and she belonged to blood group B Rhesus. During the surgery (Case 1 Figures 1-3), a single intramural myoma measuring about 18 cm by 16 cm and weighing 600 gm was excised. To execute a myomectomy, the incision was expanded laterally. The estimated blood loss was 900 ml; however, no blood transfusion was required. The operation lasted for 47 minutes. The procedure went well, and a healthy baby boy weighing 2200 gm with an APGAR score of 9 after one minute and 10 after five minutes was born without complications. To prevent severe bleeding, the patient’s uterine closure was done in layers and was given 10 IU of oxytocin intramuscularly, followed by 20 IU of oxytocin in 500 ml of Hartmann solution for 4 hours following birth, and 800 micrograms of Misoprostol were given rectally.
The patient’s postoperative recovery in the ward for postoperative care went without incident. The wound had a good healing prognosis; four days later, the patient was discharged from the ward with a normal uterine involution and a haemoglobin level of 10.8 g/dl. The patient returned for postoperative follow-up appointments on the seventh, fourteenth, and Forty-twoth days after giving birth. She had no complications on all three postoperative follow-up visits and was discharged from the clinic without any difficulties on the last postoperative follow-up visit.
Case 2: A 31-year-old primigravida an employed woman reported at our hospital at a gestation age of 38 weeks as a referral from a dispensary due abnormal pregnancy with uterine mass. On arrival she was evaluated by an ultrasound and found to have single living foetus with a cephalic presentation, an estimated weight of 3600 gm, an estimated gestation age of 40 weeks with multiple myomas and placental calcification grade three and the amniotic fluid index was 20 cm. Her full blood count revealed hemoglobin of 13 g/dl and platelets were 196, she was blood group A rhesus positive, the random blood glucose was 5.4 mmol/l and she was tested for HIV and hepatitis B and C and all tests were non-reactive. The woman was hospitalised in the antenatal ward 16th December 2023. The patient had five prenatal checkups and was not HIV or Malaria positive, she was not tested for syphilis. Despite undergoing hematinics, deworming, and Intermittent Preventive Treatment for Malaria, she was anaemic throughout all antenatal visits and the last antenatal hemoglobin level was 10.4 g/dl. She had never had any ultrasound done before during all the antental visits.
A patient underwent an elective caesarean section. Before the surgery, the anaesthetist reviewed the patient’s condition all parameters were stable for surgery. During the surgery through Pfannenstiel incision (case 2 Figures 4,5), a huge intramural myoma measuring about 10 cm by 12 cm was noted on the posterior uterine wall and other multiple intramural myomas over the posterior and anterior uterine walls including the lower segment of the uterus. A lower segment uterine incision was made a live baby girl 3.4 kg with an APGAR score of 8-10 was delivered. To execute a myomectomy, a longitudinal incision on the posterior uterine wall was made to remove the huge myoma and several incisions on the posterior and anterior walls of the uterus to remove other small myomas were made. The hemostasis was achieved by the repair of myoma and caesarean incision. The uterine compression sutures (Hayman sutures), intravenous tranexamic acid 1 g, per rectal misoprostol 800mcg and intravenous oxytocin 20IU in 500 mls of ringers’ lactate to run for 4 hrs were provided to Prevent Postpartum Hemorrhage (PPH). The estimated blood loss was 800 ml; however, no blood transfusion was required. The operation lasted for 60 minutes.
The patient’s postoperative recovery in the ward for postoperative care was uneventful. The wound had a good healing and she had no incident of postpartum hemorrhage; seven days later, the patient was discharged from the ward with a normal uterine involution and a haemoglobin level of 11.2 g/dl. The patient returned for postoperative follow-up appointments on the seventh, fourteenth, and Forty-two days postpartum with no complications on all postoperative follow-up visits and was discharged from the clinic.

Figure 1: Repair of myomectomy scar.

Figure 2: Myoma after caesarean myomectomy.
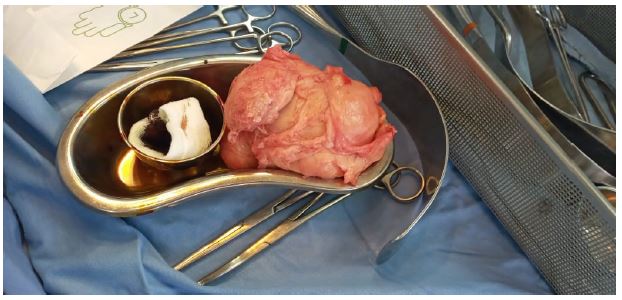
Figure 3: Prepared myoma specimen for histopathology analysis.

Figure 4: Myomectomy post caesarean section.

Figure 5: Placenta and myomas post caesarean section.
Discussion/Conclusion
Due to potential hazards, the practise of Caesarean Myomectomy in obstetrics has caused criticism throughout the years [7]. However, the procedure has shown success in selected cases, particularly when performed by experienced surgeons and in tertiary hospitals with readily available blood transfusion services [6-11]. Our case study featured a non-selected emergency and a selected (elective) case in which an experienced obstetrician successfully performed a Caesarean Myomectomy in a non-tertiary hospital with blood transfusion capabilities. Despite prior reports that the treatment can increase surgery time [10], our experience revealed no significant increase in surgery time when compared to a non-myoma Caesarean birth. Furthermore, we were able to accomplish an intramural myomectomy, which was previously thought to be impossible with a Caesarean myomectomy [9].
A Caesarean myomectomy may be required because a myoma's size and position make a Caesarean section more difficult [13]. However, it doesn't seem that postoperative issues are correlated with the size of the myoma. The Caesarean delivery procedure were made more difficult in our instance because the myoma was located in the anterior lower region in the first case and in the second case there were multiple myomas in different areas. But when compared to a non-myoma Caesarean birth, as reported in the majority of cases [12,10]. No appreciable difference in complications was seen in all these two cases. In order to reduce the risk of problems and the need for additional surgery to the patients, as we did in our situation, a Caesarean myomectomy may be performed on women during the initial treatment when possible and in the presence of a skilled surgeon as this practice has been advised in several research studies and documented cases [11,13].
Conclusion
Although it is uncommon, conducting a myomectomy during a caesarean delivery can be just as safe as doing caesarean section alone. Cesarean myomectomy for primigravidae avoids the need for two separate procedures and associated treatment costs in regions with limited resources, like Africa, where leiomyomas are common. This procedure is especially recommended in presence of experienced surgeon when the size and positioning of the fibroids make a caesarean section challenging and it can be safely done with no need of blood transfusion if postpartum management with oxytocics, tranexamic acid and application of uterine compression sutures are applied during surgery.
Acknowledgements: We appreciate the contributions of nursing, laboratory, radiology and pharmacy staff for their cooperation to achieve the best outcome of the managed cases.
References
- Laughlin SK, Baird DD, Savitz DA, Herring AH, Hartmann KE. Prevalence of uterine leiomyomas in the first trimester of pregnancy: An ultrasound screening study. Obstetrics and Gynecology. 2009; 113(3): 630.
- Michels KA, Edwards DRV, Baird DD, Savitz DA, Hartmann KE. Uterine leiomyomata and cesarean birth risk: A prospective cohort with standardized imaging. Annals of Epidemiology. 2014; 24(2): 122-126.
- Moses V, Dalal N. Pregnancy outcome in elderly primi gravidas. International Journal of Reproduction, Contraception, Obstetrics and Gynecology, 2016; 5(11): 3731-3736.
- Murmu S. Successful Myomectomy During Caesarean Section: A Case Report. 2019.
- Mahendru R, Sekhon PK, Gaba G, Yadav S. At times, myomectomy is mandatory to effect delivery. Annals of Surgical Innovation and Research, 2011; 5(1): 1-3.
- Souidan I. Is Myomectomy during Caesarean Section a Safe Procedure? Prospective Cohort Study. Benha Medical Journal. 2005; 81-88.
- Tinelli A, Nezhat CH, Likić-Ladjević I, Andjić M, Tomašević D, et al. Myomectomy during cesarean section or non-caesarean myomectomy in reproductive surgery: This is the dilemma. Clinical and Experimental Obstetrics & Gynaecology. 2021; 48(6): 1250-1258.
- Sulayman HU, Avidime S, Adesiyun AG, Ameh N, Ojabo AO, et al. Elective cesarean myomectomy: A report of two cases. Archives of International Surgery. 2013; 3(2): 189.
- Elagwany AS. Is it safe to perform caesarean myomectomy? Our experience in El-Shatby Maternity University Tertiary Hospital with review of literature. Progresos de Obstetricia y. Ginecología: Revista Oficial de La Sociedad Española de Ginecología y Obstetricia.2017; 60(5): 428-431
- Sultana R, Noor S, Nazar AF, Abbasi N, Bashir R, et al. Safety of caesarean myomectomy. Journal of Ayub Medical College Abbottabad, 2021; 24(2): 120-121.
- Ramya T, Sabnis SS, Chitra TV, Panicker S. Cesarean myomectomy: An experience from a tertiary care teaching hospital. The Journal of Obstetrics and Gynecology of India. 2019: 69: 426-430.
- Zhao R, Wang X, Zou L, Zhang W. Outcomes of Myomectomy at the Time of Cesarean Section among Pregnant Women with Uterine Fibroids: A Retrospective Cohort Study. BioMed Research International. 2019; 7576934. https://doi.org/10.1155/2019/7576934
- Onyekpa IJ, Odugu BU, Nevo C. Unavoidable Caesarean Myomectomy Due to Multiple Anterior Uterine Fibroids: A Case Report. J Med-Clin Res & Rev. 2020; 6(7): 1-3.
