
Open Access, Volume 10
Intravenous liposomal amphotericin B efficacy and safety for localized cutaneous leishmaniasis: Case series
Gaia Fasano1,2*; Domenico D’amico1; Giancarlo Valenti1
1Department of Dermatology, University Hospital, “Renato Dulbecco”, Catanzaro, Italy.
2Magna Graecia University, Catanzaro, Italy.
Gaia Fasano
Departement of Dermatology, University Hospital, “Renato Dulbecco”, Catanzaro, Italy.
Email: fasano.gaia@gmail.com
Received : June 13, 2024,
Accepted : June 28, 2024
Published : July 10, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Background: Cutaneous Leishmaniasis (CL) is a skin infection caused by several Leishmania parasites transmitted through sandfly bites, characterized mostly by skin nodules and ulcers in affected individuals. Leishmaniasis is present in the tropical and subtropical temperate areas of the world and throughout the Mediterranean region, particularly in the southern Italian regions such as Calabria and Sicily.
Intravenous Liposomal Amphotericin B (IV L-AmB) is the most effective therapeutic agent for the visceral form of leishmaniasis, but its utilization is growing also for CL.
Methods: Here we report the clinical features and images of four patients affected by localized CL due to Leishmania major, successfully treated with IV L-AmB.
Results: We observed four patients (3M, 1F, average age: 69 years) with localized CL initially presenting with different skin lesions (e.g. erythematous plaques, papules, or ulcerated lesions), treated with IV L-Amb 3 mg/kg/day infusion from day 1 to day 5 followed by one infusion on day 10 after the failure of local or systemic treatments. An excellent clinical improvement was recorded in all patients, with only a singular infusion reaction and transitory gastrointestinal side effects. No relapses were found in all patients, during the follow-up period (maximum of 5 years).
Conclusion: Our case series confirms that CL can present with various and challenging clinical manifestations. Our results suggest that IV L-AmB could be a promising and safe systemic therapy in CL caused by L. major.
Keywords: Cutaneous leishmaniasis; Leishmania major; Intravenous liposomal amphotericin B.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Fasano G (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Fasano G, D’amico D, Valenti G. Intravenous liposomal amphotericin b efficacy and safety for localized cutaneous leishmaniasis: Case series. Open J Clin Med Case Rep. 2024; 2260.
Introduction
Leishmaniasis is a parasitic disease caused by protozoa of the genus Leishmania, transmitted by sand fly vectors. Human leishmaniasis involves over 20 distinct species, with infections geographically distributed between the Old World (Mediterranean, Middle East, Africa, and Asia) and the New World (Americas) [1].
Different forms of leishmaniasis encompass Cutaneous Leishmaniasis (CL), Mucosal Leishmaniasis (ML) and Visceral Leishmaniasis (VL). CL involves localized forms (LCL) and rarer diffuse forms (DCL). Common clinical presentations are singular or multiple lesions often occurring in the exposed areas of the skin, including pink papules, nodules, plaque lesions and painless chronic ulcers [2]. Symptomatic CL can manifest after an incubation period from weeks to months [3]. The natural progression of LCL comprises the development of an atrophic and depressed scar or complete healing over months or years [4].
The diagnosis and treatment of LCL are challenging due to the need for standardized laboratory techniques and specialized physicians [5].
Local therapy, such as paromomycin 15% cream or intralesional pentavalent antimonials, are a reasonable option for uncomplicated CL. Systemic therapy is warranted in complicated CL, immunocompromised individuals, chronic lesions, and patients with increased risk factors for ML [6]. Some studies showed that antifungal azoles (fluconazole and itraconazole) can be effective against CL [7]. Intravenous agents for CL include pentavalent antimonials, Liposomal Amphotericin B formulation (L-AmB), and pentamidine. Historically, pentavalent antimonials have been the gold standard parenteral therapy of CL [8]. However, antimonials are not commercially available for human use in Italy anymore. Previously, L-AmB was exclusively used for VL treatment. Recent years have shown its clinical effectiveness in CL as well, making it an emerging option for CL therapy [9,10]. Here we report four CL cases successfully and safely treated with intravenous (i.v.) L-AmB.
Case Series
Case 1: A 57-year-old male initially presented with a one-year-old pink-coloured papule on his left leg. Over time, the papule enlarged and formed a plaque-like lesion with a central softening. It was surrounded by a distinct, raised and hardened border with a painless ulceration at the center. Small satellite lesions surrounded the ulcer (Figure 1). There were no systemic symptoms like fever, asthenia and malaise. Skin biopsy revealed the presence of parasites inside macrophages suggesting Leishmania infection. Quantitative Polymerase Chain Reaction (PCR) disclosed L. major species. Therefore, a diagnosis of LCL was made. The patient underwent topical paramomycin 15% once daily for one month with no clinical improvement. After obtaining informed consent, a subsequent therapy with i.v. L-AmB 3 mg/kg/day infusion from day 1 to day 5 followed by one infusion on day 10 determined remarkable improvement. At the end of three months, the lesion completely healed, showing only post-inflammatory hyperpigmentation (Figure 2). No adverse events were reported during the treatment. No clinical relapses were observed during the two-year follow-up.

Figure 1: Clinical image.

Figure 2: Clinical image.
Case 2: A 69-year-old woman reported a six-month history of a single painless erythematous papule on her nose and upper eyelid, which progressively worsened into a large erythematous and edematous area without satellite papules. At the time of our first observation, we noted a broad infiltrated plaque with irregular margins sparing mucocutaneous areas (Figure 3). The LCL diagnosis was confirmed by staining a smear from a tissue fragment at the ulcer’s edge with May-Grunwald-Giemsa (MGG). Leishmania parasites were evident inside the cytoplasm of histiocytic cells. PCR revealed L. major species. She was treated with topical paromomycin cream 15% once daily for 1 month with no improvement. Hence, after obtaining informed consent, the therapy with IV L-AmB 3 mg/kg/day infusion from day 1 to day 5 followed by one infusion on day 10 determined the complete healing of the affected area, with reduced swelling and mild erythema. Only a post-inflammatory hyperpigmentation persisted after three months (Figure 4). No adverse events occurred during the treatment and no new recurrences were reported during the 3-year follow-up period.
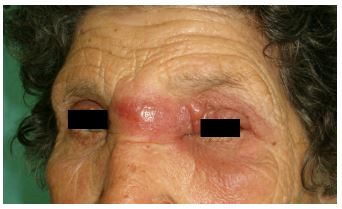
Figure 3: Clinical image.
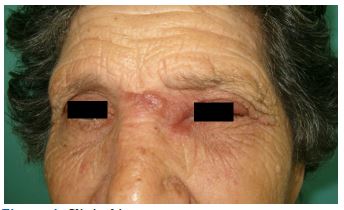
Figure 4: Clinical image.
Case 3: An immunocompromised 82-year-old man had a history of colorectal cancer treated with chemotherapy. Approximately 6 months before presentation, he developed an erythematous plaque on the right cheek extending to the right temporal region and forehead, with overlying crusting and ulceration (Figure 5). The lesion was pruritic and not painful. The skin examination revealed normal underlying mucosa. Over the past few months, the lesion had been incorrectly treated with topical corticosteroids with progressive enlargement over time. A skin biopsy performed on the right cheek showed pseudoepitheliomatous hyperplasia of the epidermis with a polymorphic inflammatory granuloma consisting of epithelioid and plasma cells. PCR confirmed L. major species and the diagnosis of an extensive facial CL was made. The patient was initially treated with itraconazole 200 mg per day for 3 weeks without improvement. Subsequently, after obtaining informed consent, IV L-AmB therapy was initiated at a dosage of 3 mg/kg/day infusion from day 1 to day 5 followed by one infusion on day 10. The patient reported a possible infusion reaction characterized by the onset of arterial hypotension and a brief loss of consciousness. The infusion speed was slowed for the subsequent infusions and no more adverse events were noted. After 3 months, we observe the partial resolution of the inflammation with mild residual erythema without crusts or ulcers (Figure 6). No recurrences were recorded during the following 5 years.

Figure 5: Clinical image.

Figure 6: Clinical image.
Case 4: A 68-year-old man, who has a history of psoriatic arthritis treated with adalimumab, presented with an ulcerated skin lesion on the scalp slowly growing for 8 months, preceded by an insect bite one year earlier. Upon skin examination, we observed an ulcerated nodule associated with swelling in the right parietal region (Figure 7). There were no signs or symptoms of systemic involvement. RT-PCR analysis on a punch biopsy specimen tested positive for L. major species, making the diagnosis of LCL definitive. Adalimumab therapy was discontinued. The itraconazole 200 mg per day for 3 weeks therapy initially administered did not yield any improvement, prompting the introduction, after obtaining informed consent, of IV L-AmB therapy at a dosage of 3 mg/kg/day infusion from day 1 to day 5 followed by one infusion on day 10, leading to complete resolution of the ulcer within two months (Figure 8). The patient reported nausea and vomiting during the early stages of the infusions, which resolved at the end of the therapy. No recurrences were reported during the next five years of follow-up.

Figure 7: Clinical image.

Figure 8: Fluoroscopy showing the position of the central
Table 1: Demographic and clinical features of our CL cases.
| Case | Patient demographics | Immuno-compromised state | Clinical features | Leishmania complex | Treatment regimen | Follow-up Range, mo | Adverse reactions |
|---|---|---|---|---|---|---|---|
| 1 | M, 57 y | No | LCL on the left leg | L. major | Topical paromomycin cream 15% followed by IV L-AmB | 24-Jan | No |
| 2 | F, 69 y | No | LCL on the nose and upper eyelid | L. major | Topical paromomycin cream 15% followed by IV L-AmB | Jan-36 | No |
| 3 | M, 82 y | Yes | Extensive facial CL | L. major | Itraconazole per os followed by IV L-AmB | Jan-60 | Infusion reaction |
| 4 | M, 68 y | No | Ulcerated CL on the scalp | L. major | Itraconazole per os followed by IV L-AmB | Jan-60 | GI symptoms |
LCL: Localized Cutaneous Leishmaniasis; CL: Cutaneous Leishmaniasis; L. Major: Leishmania Major; IV L-AmB: Intravenous Liposomal Amphotericin B; GI: Gastrointestinal.
Discussion
We documented four patients referring to our Dermatology department with different clinical manifestations of CL due to L. major successfully treated with IV L-AmB. Demographic and clinical features of our CL cases are presented in Table 1. Amphotericin B (AmB) disrupts fungal cell membranes by interacting with ergosterol, causing ion leakage and cell death. It was considered second-line therapy for CL and MCL during the 1960s. Its use was limited due to renal toxicity, systemic effects, costs, and logistical difficulties in endemic areas [11]. The liposomal form of AmB is preferred due to its reduced toxicity compared to the conventional deoxycholate form [12]. Wortmann et al. [13] observed an 84% response rate among a cohort of 20 patients diagnosed with CL caused by different parasite strains, treated with a regimen of 3 mg/kg/day of L-AmB over 21 days. Guery et al. [14] suggested that L. infantum species may be more susceptible to L-AmB, but also individual factors such as age, immunosuppression state and comorbidities should be considered [14]. Senchaya et al [15]. Reported a higher response rate (72%) in CL treated with short-term L-AmB therapy, leading to shorter hospitalization periods. Lemieux et al. [16] reported a response rate of 69% in 48 patients with CL. Among various studies, the most frequent adverse effects included urticarial rash, acute kidney injury, nausea and vomiting [17]. L-Amb may cause infusion-related reactions such as flank/abdominal pain, chest discomfort, and dyspnea [13-20]. The majority of the current studies documented the efficacy of L-AmB for CL related to L. tropica or L. infantum, while limited evidence is available for L. major [11,21,22].
Our case series highlighted the efficacy and tolerability of IV L-AmB as a second-line treatment in CL due to L. major, confirming the occurrence of only a few adverse events in 2 patients (mild infusion reactions, nausea and vomiting). No patients had to interrupt prematurely the treatment.
All patients underwent regular follow-ups for at least two years because of the well-known risk of relapses on the site of the primary ulcer [23].
Conclusion
Our study examining mild-to-moderate CL cases suggests that intravenous L-AmB may serve as an effective and safe treatment in CL caused by L. major, even after the failure of prior therapies. Therefore, since antimonials are not commercially available for human use in Italy anymore, intravenous L-AmB could potentially become a first-line therapy in the future.
References
- Chivinski J, Nathan K, Naeem F, Ekmekjian T, Libman MD, et al. Intravenous Liposomal Amphotericin B Efficacy and Safety for Cutaneous and Mucosal Leishmaniasis: A Systematic Review and Meta-analysis. Open Forum Infect Dis. 2023; 10(7): ofad348. Published 2023 Jul 11. doi:10.1093/ofid/ofad348
- Melby PC. Experimental leishmaniasis in humans: review. Rev Infect Dis. 1991; 13(5): 1009-1017. doi:10.1093/clinids/13.5.1009
- Follador I, Araújo C, Bacellar O, et al. Epidemiologic and immunologic findings for the subclinical form of Leishmania braziliensis infection. Clin Infect Dis. 2002; 34(11): E54-E58. doi:10.1086/340261
- Dowlati Y. Cutaneous leishmaniasis: clinical aspect. Clin Dermatol. 1996; 14(5): 425-431. doi:10.1016/0738-081x (96)00058-2
- Herwaldt BL, Arana BA, Navin TR. The natural history of cutaneous leishmaniasis in Guatemala. J Infect Dis. 1992; 165(3): 518-527. doi:10.1093/infdis/165.3.518
- Blum J, Buffet P, Visser L, et al. LeishMan recommendations for treatment of cutaneous and mucosal leishmaniasis in travelers, 2014. J Travel Med. 2014; 21(2): 116-129. doi:10.1111/jtm.12089
- Aronson N, Herwaldt BL, Libman M, et al. Diagnosis and Treatment of Leishmaniasis: Clinical Practice Guidelines by the Infectious Diseases Society of America (IDSA) and the American Society of Tropical Medicine and Hygiene (ASTMH). Clin Infect Dis. 2016; 63(12): e202-e264. doi:10.1093/cid/ciw670
- Emad M, Hayati F, Fallahzadeh MK, Namazi MR. Superior efficacy of oral fluconazole 400 mg daily versus oral fluconazole 200 mg daily in the treatment of cutaneous leishmania major infection: a randomized clinical trial. J Am Acad Dermatol. 2011; 64(3): 606-608. doi:10.1016/j.jaad.2010.04.014
- Palumbo E. Treatment strategies for mucocutaneous leishmaniasis. J Glob Infect Dis. 2010; 2(2): 147-150. doi:10.4103/0974-777X.62879
- Frézard F, Aguiar MMG, Ferreira LAM, et al. Liposomal Amphotericin B for Treatment of Leishmaniasis: From the Identification of Critical Physicochemical Attributes to the Design of Effective Topical and Oral Formulations. Pharmaceutics. 2022; 15(1): 99. doi:10.3390/pharmaceutics15010099
- Shirzadi MR. Lipsosomal amphotericin B: A review of its properties, function, and use for treatment of cutaneous leishmaniasis. Res Rep Trop Med. 2019; 10: 11-18. doi:10.2147/RRTM.S200218
- Mistro S, Maciel Ide M, de Menezes RG, Maia ZP, Schooley RT, et al. Does lipid emulsion reduce amphotericin B nephrotoxicity? A systematic review and meta-analysis. Clin Infect Dis. 2012; 54(12): 1774-1777. doi:10.1093/cid/cis290
- Wortmann G, Zapor M, Ressner R, et al. Lipsosomal amphotericin B for treatment of cutaneous leishmaniasis. Am J Trop Med Hyg. 2010; 83(5): 1028-1033.
- Guery R, Henry B, Martin-Blondel G, et al. Liposomal amphotericin B in travelers with cutaneous and muco-cutaneous leishmaniasis: Not a panacea. PLoS Negl Trop Dis. 2017; 11(11): e0006094. doi: 10.1371/journal.pntd.0006094
- Senchyna A, Simon S, Cissé H, et al. American cutaneous leishmaniasis in French Guiana: a retrospective comparison between liposomal amphotericin B and meglumine antimoniate. Br J Dermatol. 2020; 183(2): 389-391. doi:10.1111/bjd.18964
- Lemieux A, Lagace F, Billick K, et al. Cutaneous leishmaniasis: A 10- year experience in a Canadian reference centre for tropical diseases. J Am Acad Dermatol. 2019; 81: AB40.
- Solomon M, Pavlotsky F, Leshem E, Ephros M, Trau H, et al. Liposomal amphotericin B treatment of cutaneous leishmaniasis due to Leishmania tropica. J Eur Acad Dermatol Venereol. 2011; 25(8): 973-977. doi: 10.1111/j.1468-3083.2010.03908.x
- Roden MM, Nelson LD, Knudsen TA, et al. Triad of acute infusion-related reactions associated with liposomal amphotericin B: Analysis of clinical and epidemiological characteristics. Clin Infect Dis. 2003; 36(10): 1213-1220. doi:10.1086/374553
- Rodríguez Galvis MC, Pérez Franco JE, Casas Vargas MY, Ordoñez Rubiano MF. Effectiveness and Safety of Amphotericin B Deoxycholate, Amphotericin B Colloidal Dispersion, and Liposomal Amphotericin B as Third-Line Treatments for Cutaneous and Mucocutaneous Leishmaniasis: A Retrospective Study. Am J Trop Med Hyg. 2020; 102(2): 274-279. doi:10.4269/ajtmh.18-0514
- Lemieux A, Lagacé F, Billick K, et al. Cutaneous leishmaniasis in travellers and migrants: A 10-year case series in a Canadian reference centre for tropical diseases. CMAJ Open. 2022; 10(2): E546-E553. doi:10.9778/cmajo.20210238
- Mosimann V, Neumayr A, Paris DH, Blum J. Liposomal amphotericin B treatment of Old World cutaneous and mucosal leishmaniasis: A literature review. Acta Trop. 2018; 182: 246-250. doi: 10.1016/j.actatropica.2018.03.016
- Ramos GS, Vallejos VMR, Borges GSM, et al. Formulation of Amphotericin B in PEGylated Liposomes for Improved Treatment of Cutaneous Leishmaniasis by Parenteral and Oral Routes. Pharmaceutics. 2022; 14(5): 989
- Marovich MA, Lira R, Shepard M, et al. Leishmaniasis recidivans recurrence after 43 years: A clinical and immunologic report after successful treatment. Clin Infect Dis. 2001; 33(7): 1076-1079. doi:10.1086/322643
